|
|
 |
Back to 2011 Program
THE IMPACT OF FIBERWIRE, FIBERLOOP AND LOCKING SUTURE CONFIGURATION ON FLEXOR TENDON REPAIRS.
Ludmila Haimovici, D.O.1, Sotirios Papafragkou, M.D.2, Jason Adams, D.O.1, Alexander B. Dagum, M.D.3.
1St Barnabas Hospital, Bronx, NY, USA, 2University of Medicine and Dentistry of New Jersey, Newark, NJ, USA, 3Stony Brook Medical Center, Stony Brook, NY, USA.
BACKGROUND:
Early active motion, new suture technique and material have all led to improved outcomes in flexor tendon repair. Fiberwire (Arthrex, Naples, FL) suture with its superior strength and stiffness has gain widespread popularity among hand surgeons performing flexor tendon repair. Increasing the number of strands, size of suture and decreasing the number of knots and bulk all lead to increase strength in the tendon repair. The recent innovation of Fiberloop suture a double-stranded needle with Fiberwire suture provides an opportunity to double the number of strands across the repair site without increasing the bulk and the number of knots.We evaluated the contribution to the tensile strength of flexor tendon repair using the strongest suture material, Fiberwire, and the best surgical technique (locking configuration) utilizing two and four-strand core repair. Our null hypothesis was that there would be no difference between a four strand 4-0 Fiberwire double Pennington repair, 4-0 Fiberloop and 2-0 Fiberwire single Pennington repair.
METHODS: Thirty flexor digitorum profundus tendons were harvested from fresh-frozen human cadaver hands and randomized to 3 groups of ten tendons each. All tendons were repaired using locking configuration (as derived from Pennington's report) as follows: (1) 4-strand suture single repair with 4-0 Fiberloop, (2) 4-strand suture double repair with 4-0 Fiberwire, (3) 2-strand suture repair with 2-0 Fiberwire (Fig. 1). Load-to-failure testing was performed using Instron Material Testing Machine, visible 2 mm gap and maximum tensile strength were statistically analyzed
RESULTS: The mode of failure for all core sutures in each technique was a pull-out. The maximum tensile strength for all 3 experimental groups is listed in Table 1. There was a significant difference among the two different four-strand repairs (p < .001). In post hoc testing 4-0 Fiberwire (double-Pennington) repair was found to be significantly stronger than 4-0 Fiberloop (single-Pennington) repair (p < .001). When the two-strand repair (2-0 Fiberwire) was compared to four-strand single Pennington repair (4-0 Fiberloop) there was no significant difference found (p <.14). Assessment of the visible 2-mm gap forces using a 2-factor ANOVA showed a significant difference among the 3 different groups being compared. 4-0 Fiberwire (double-Pennington) repairs in general was found to sustain a significantly higher 2-mm gap force than both 4-0 Fiberloop and 2- 0 Fiberwire repairs (p < .048). No significant differences in 2-mm gap testing were found between 4-0 Fiberloop and 2-0 Fiberwire (p <. 40).
CONCLUSIONS: • Suture material, and the number of strands play a critical role in achieving optimal strength of flexor tendon repairs,
• Suture technique (specifically how you pass the suture strands across the repair site) yields the greatest value in achieving maximum tensile strength with reduced gapping at the repair site.
Suture material and strenght| Suture Material | Max Tensile strength of suture material alone, N | Max Tensile strength of repair at suture failure, N | Visible gap force, N | Failure mode, n | | 4-0 Fiberwire | 15 + -2 | 56 + - 2 | 28.5 + - 3 | 10 | | 4-0 Fiberloop | 34 + - 3 | 32.8 + - 4 | 21.4 + - 3 | 10 | | 2-0 Fiberwire | 52 + -3 | 37 + - 2 | 24.4 + - 2 | 10 | 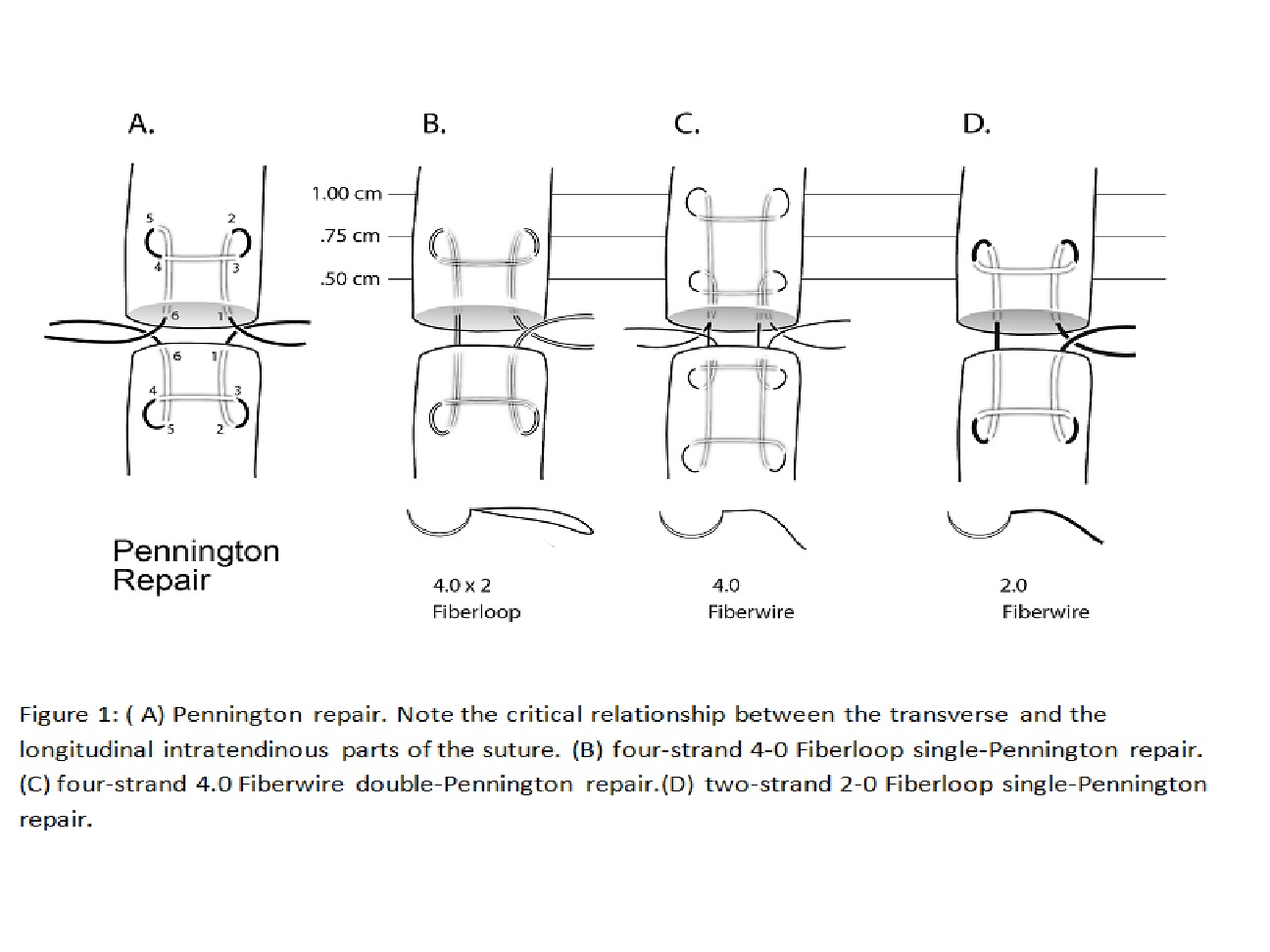
Back to 2011 Program
|







