Back to 2014 Annual Meeting Abstracts
A Quantitative Analysis of Facial Asymmetry in Congenital Muscular Torticollis (CMT) Using Three-Dimensional Photogrammetry
Vanessa M. Baratta, BA, Olivia E. Linden, BA, Margaret E. Byrne, RN, Stephen R. Sullivan, MD, MPH, Helena O. Taylor, MD, PhD.
Brown, Providence, RI, USA.
Background: Congenital muscular torticollis (CMT) is a condition in which an infant’s head is tipped to one side, while the chin is turned to the other secondary to asymmetric forces of the neck musculature. CMT affects 0.3-2% of live births, most frequently arising from sternocleidomastoid muscle damage (1). Facial asymmetry can result from persistent CMT, though the evolution of this asymmetry is poorly characterized. Past studies used computed tomography (CT) to evaluate craniofacial skeletal asymmetry, but the soft tissues could not be evaluated in this manner (2). With three-dimensional (3D) imaging systems, surface features of soft tissue can be quantitatively assessed. We previously used 3D photogrammetry to quantify facial surface asymmetry as a numeric value, known as the root mean square deviation (RMSD) (3). The purpose of this study is to quantitatively evaluate facial surfaces in patients with CMT and compare them to age-matched controls to better characterize the patterns of soft tissue asymmetry resulting from torticollis.
Methods: 13 pediatric patients diagnosed with CMT and 13 age-matched volunteers underwent 3D photogrammetry of their faces with the Canfield VECTRA system. RMSD is the measured difference between the native and reflected faces about a plane of maximum symmetry. We calculated the full face RMSDs of individual surface scans (Figure 1). We then calculated the RMSDs of the upper, middle, and lower facial thirds defined by the facial landmarks shown to isolate the region with greatest asymmetry. Analysis was performed by two independent examiners to calculate inter-observer reliability.
Results: Patient characteristics are shown in Table 1.
Table 1: Demographic Information| Patient Data | Controls (n=13) | CMT (n=13) | | Sex (M:F) | 0.44:1 | 1.6:1 | | Age (p=0.6) | Avg 0.5y
(0.1-1.3y) | Avg 0.4y
(0.3-1.2y) | | Race | Caucasian: 6
Black: 1
Hispanic: 5
Mixed: 1 | Caucasian:11
Hispanic: 2 | Torticollis subjects had statistically significant greater whole face, upper third and middle third facial asymmetry than age-matched controls (p<0.05, Table 2). Table 2: RMSD values in CMT and controls | Control RMSD (mean, range in mm) | CMT RMSD (mean, range in mm) | P Value | | Total face | 0.7
(0.9-1.1) | 1.1
(0.7-1.5) | p=0.0008 | | Upper face | 0.7
(0.4-1.2) | 1.0
(0.5-1.5) | p=0.0096 | | Middle face | 0.8
(0.3-1.2) | 1.1
(0.6-1.9) | p=0.0171 | | Lower face | 0.8
(0.3-1.6) | 1.2
(0.6-2.0) | p=0.0545 | Figure 2 plots whole face RMSD values in pediatric patients (red) and controls (blue). Conclusions: We used 3D photogrammetry to quantitatively assess the surface asymmetry of CMT patients. We found greater asymmetry in patients with torticollis than in their unaffected peers. All areas of the face appeared to be affected, though the asymmetry in the lower facial third just failed to reach significance. We are following patients longitudinally to better characterize this facial asymmetry and to better guide therapy. 1. Beasley S. Torticollis. In: Grosfeld JL, et. al. Pediatric Surgery, 6th ed. Mosby, 2006, P875-881. 2. Yu CC, et al. Craniofacial deformity in patients with uncorrected CMT. PRS 2004;13:24-33. 3.Taylor HO, et al. Quantitative Facial Asymmetry: using three-dimensional photogrammetry to measure baseline facial surface symmetry. JCFS 2013. 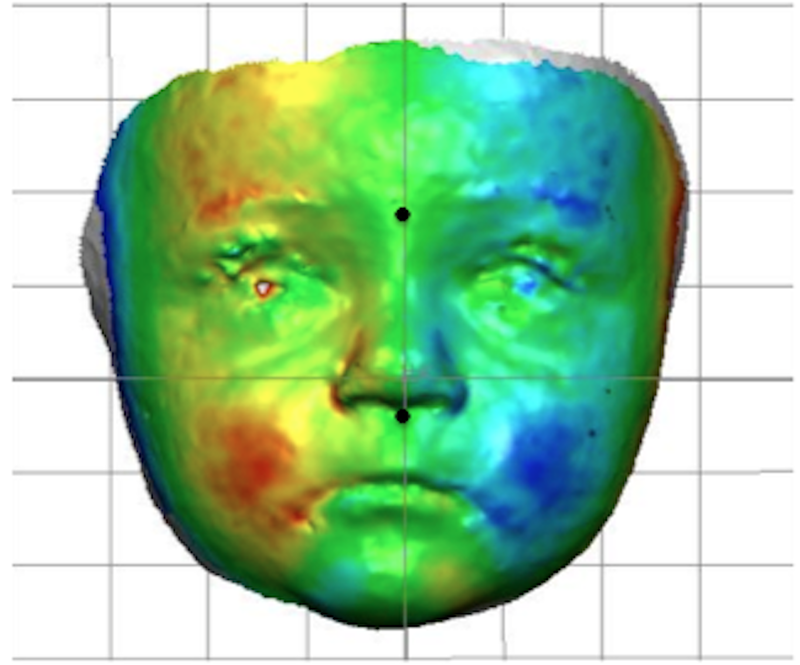 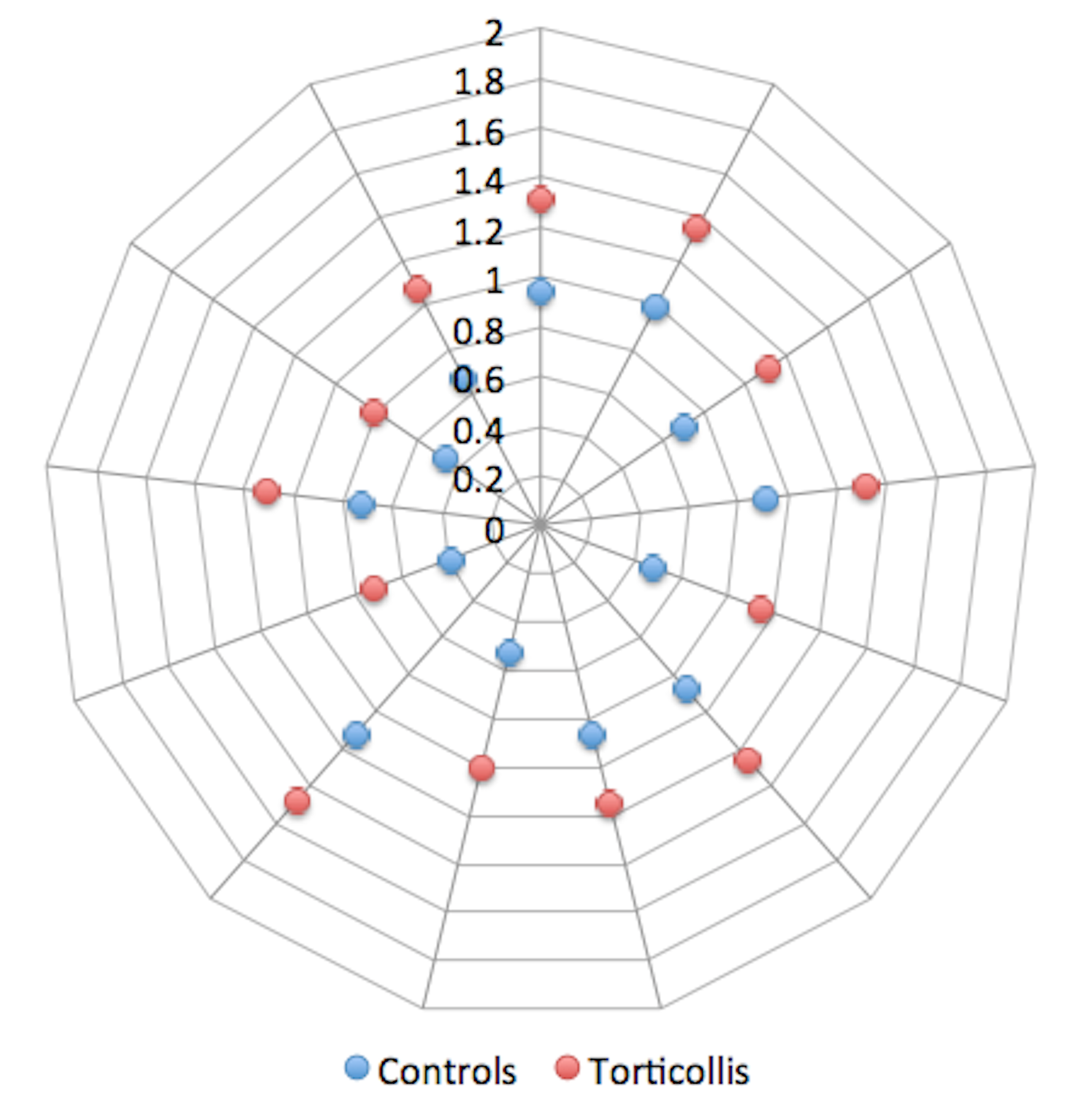
Back to 2014 Annual Meeting Abstracts
|




