Back to 2014 Annual Meeting Abstracts
Posterior Component Separation with Transversus Abdominis Release: Technique and Utility in Challenging Abdominal Wall Reconstruction Cases
Christine M. Jones, MD, John D. Potochny, MD, Eric M. Pauli, MD.
Penn State Hershey Medical Center, Hershey, PA, USA.
BACKGROUND: Ventral hernia is a frequent and challenging problem. More patients today are presenting with significant comorbidities, loss of domain, and difficult anatomic considerations. The ideal method of hernia repair has not yet been found. Non-midline hernias, parastomal hernias, and recurrent ventral hernias after traditional anterior component separation present a particular challenge to repair. In these cases, typical reconstructive techniques would struggle to reestablish abdominal domain to create a lasting repair. Posterior component separation with transversus abdominis release is a new reconstructive technique that offers a durable solution to challenging ventral hernias.
METHODS: Posterior component separation begins with a midline laparotomy incision. All adhesions to the posterior abdominal wall are taken down. A Rives-Stoppa-Wantz retro-rectus dissection is carried out, mobilizing large lateral musculocutaneous flaps. Just medial to the linea semilunaris, the transversus abdominis is released by dividing the fascia and muscle insertion to the posterior layer. This allows a wide plane of pre-peritoneal dissection. The plane extends to the psoas muscle laterally, under the costal margin to the central tendon of the diaphragm superolaterally, below the inguinal ligament inferolaterally, and to the neck of the bladder inferiorly. The perforating neurovascular bundles between the internal oblique and transversus abdominis are spared, creating well-vascularized flaps that retain contractile strength. Large sheets of mesh are placed beneath the transversus abdominis in a sublay fashion to reinforce the repair. The rectus abdominis can reliably be advanced to allow for a midline abdominal closure. This technique can be used in non-midline hernias, subxiphoid or suprapubic hernias, and in patients who previously had an anterior component separation - patients who previously had few or very difficult reconstructive options.
RESULTS: Results with posterior component separation are reliable and durable, suggesting a 5% recurrence rate at 2 years. At our institution, prospective data collection is being conducted and is thus far encouraging, as no patients have developed recurrent hernias one year after posterior component separation.
CONCLUSION: Posterior component separation is a versatile, easy-to-learn technique of hernia repair that offers a reliable, durable solution to complex abdominal wall reconstruction.
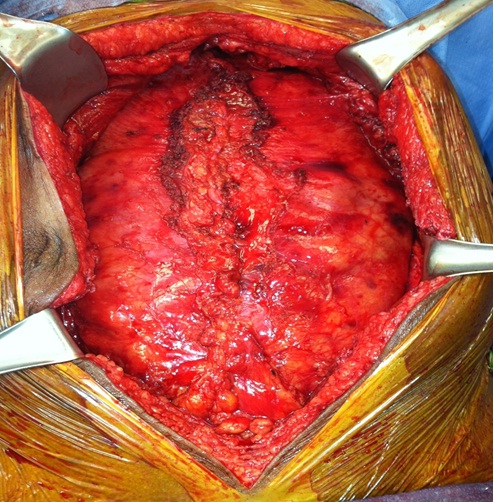
FIGURE 1: Midline closure of the posterior rectus sheath.
FIGURE 2: Mesh placement in a sublay position between the closed posterior layer and the musculature anteriorly
Back to 2014 Annual Meeting Abstracts
|




