Back to 2014 Annual Meeting Abstracts
Endoscopic-assisted infraorbital nerve release after craniofacial trauma
Michael Sosin, MD, Carla De La Cruz, BS, Michael R. Christy, MD.
R Adams Cowley Shock Trauma Center, Baltimore, MD, USA.
Background:
Visualization and exposure of the craniofacial skeleton has always been a challenge in the treatment of facial fractures. Endoscopic techniques have become widely available and applicable to multiple surgical disciplines. However, in plastic surgery and craniofacial surgery its use is limited. We present a patient with infraorbital nerve entrapment that was treated with an endoscopic-assisted nerve release of the surrounding soft tissue and circumferential foramenal osteotomy. The purpose of this case report is to describe a novel endoscopic-assisted technique that can be added to the plastic surgeon’s armamentarium in accessing craniofacial anatomy.
Methods:
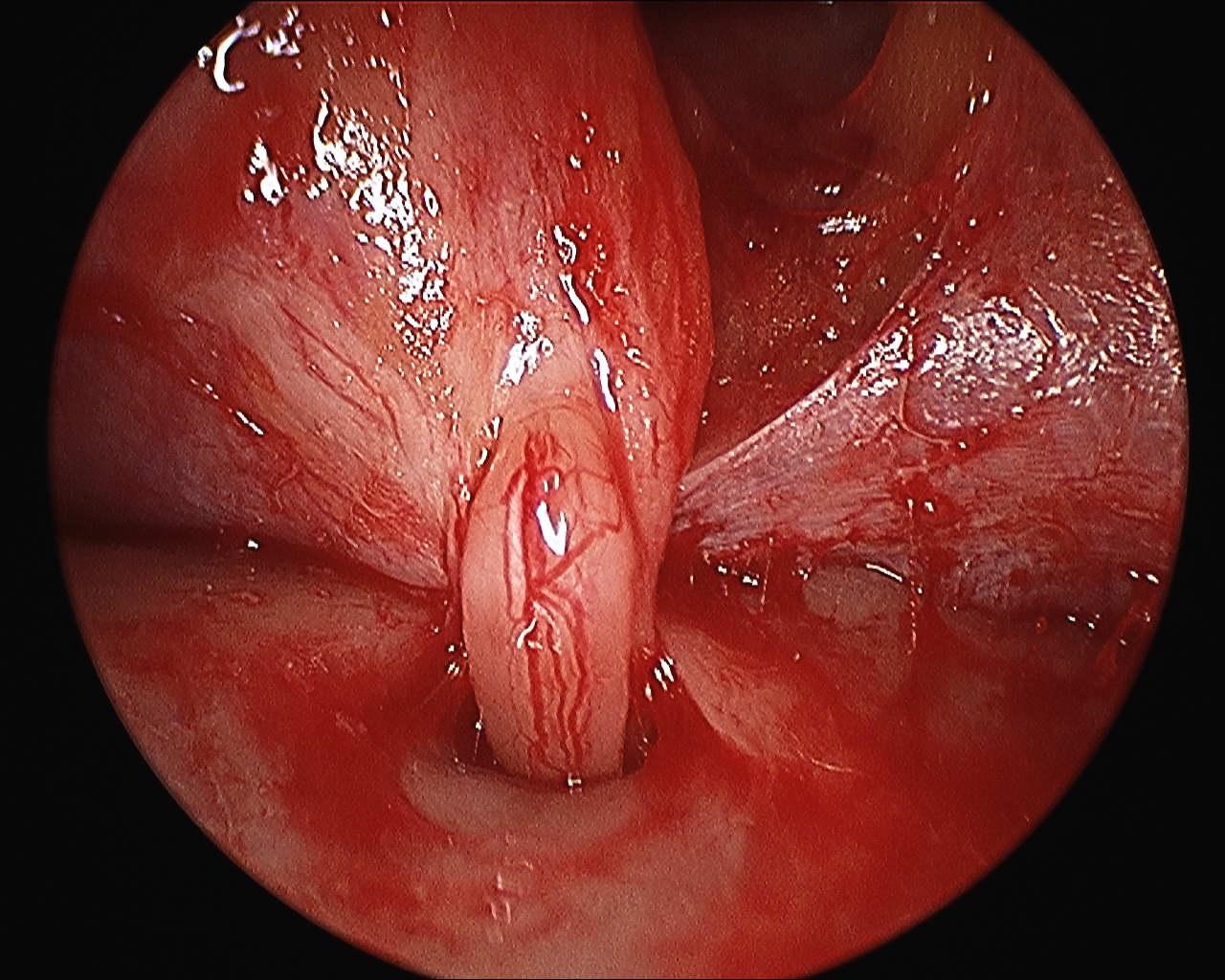
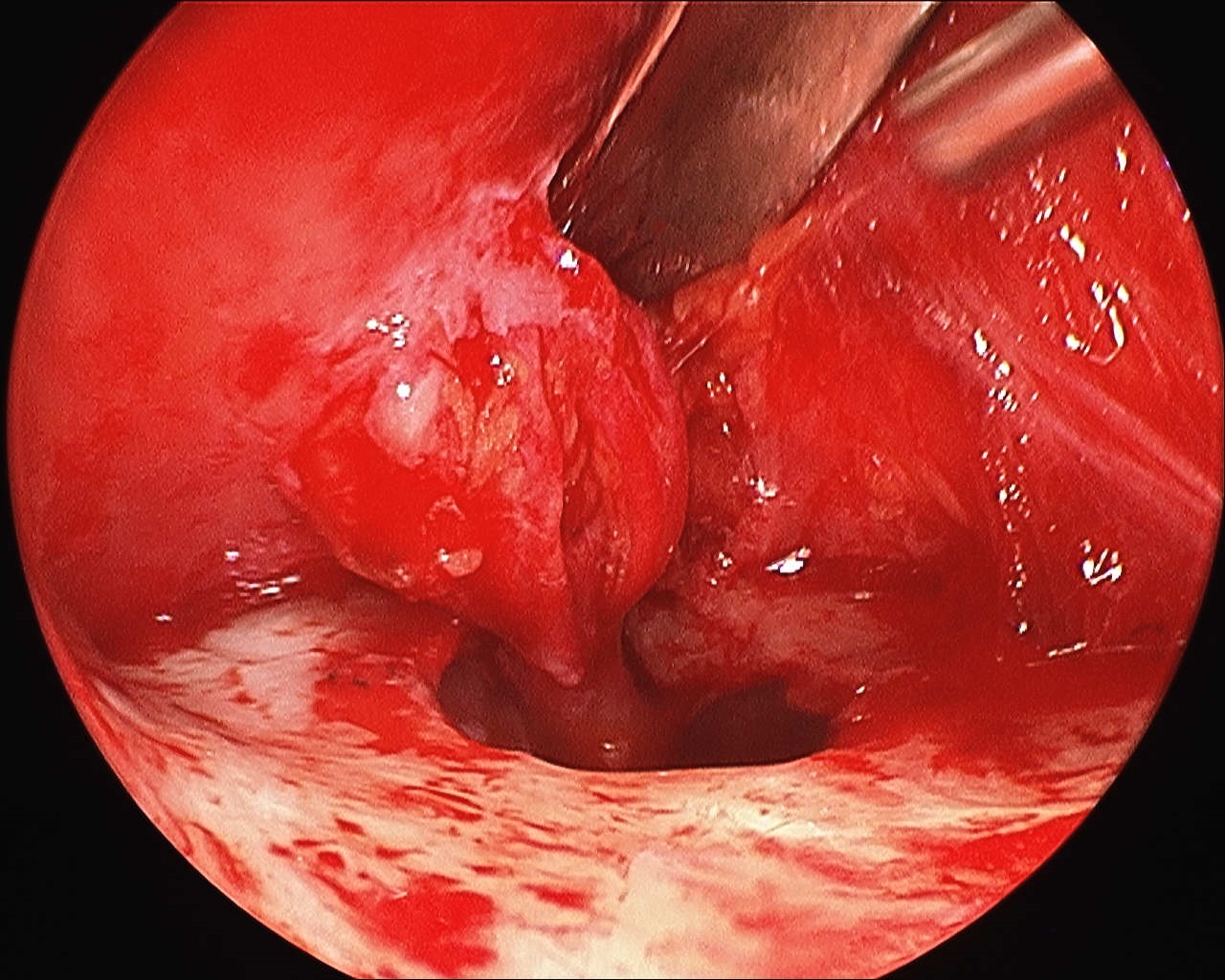
A 35-year-old Caucasian male presented to our clinic following blunt facial trauma, two month prior, resulting in a left zygomaticomaxillary complex and orbital fracture. Physical exam and radiologic examination revealed infraorbital nerve entrapment. The patient underwent an endoscopic-assisted infraorbital nerve decompression and circumferential osteotomy of the infraorbital foramen. The left upper buccal sulcus was incised and dissection was carried out in the subperiosteal plane to the maxilla. A Tessier elevator was then used to carefully lift periosteum and scar to allow access for a 30-degree endoscope (Stryker, San Jose, California). Visualization of the left infraorbital nerve and the infraorbital foramen revealed multiple soft tissue adhesions from the anterior soft tissue causing nerve compression [Figure 1]. Endoscopic visualization allowed for precise adhesiolysis using long tenotomy scissors with preservation of the nerve and its branches revealing viable neural tissue. A 1-mm osteotome was then used to perform a circumferential osteotomy of the left infraorbital foramen in a box-like fashion [Figure 2]. The endoscope was then introduced into the foramen to visualize nerve tracking posteriorly ensuring that there was no proximal impingement.
Results:
The patient reported immediate resolution of symptoms following the procedure and was discharged to home the same day of surgery. Upon 3 year follow-up, the patient remained symptom free.
Conclusion:
The novel description of an endoscopic-assisted approach to decompress the infraorbital nerve is a minimally invasive technique that provides better visualization for adhesiolysis, nerve dissection, circumferential osteotomy, and it decreases the manipulation of tissue with that of an open approach. As endoscopic techniques evolve and surgeons become more adept at incorporating endoscopy into craniofacial surgery, we advocate this approach to decompression of the infraorbital nerve.
Back to 2014 Annual Meeting Abstracts
|




