Back to 2014 Annual Meeting Posters
The Lip Nose Junction: Do current cleft lip repairs violate anatomic principles
Sebastian Brooke, MD, Mitchell Flurry, MD, Alexis Tashima, BS, Duncan Mackay, BA, Duncan Mackay, BA, Thomas Samson, MD, Donald Mackay, MD, DDS.
Penn StateHershey Medical Center, Hummelstown, PA, USA.
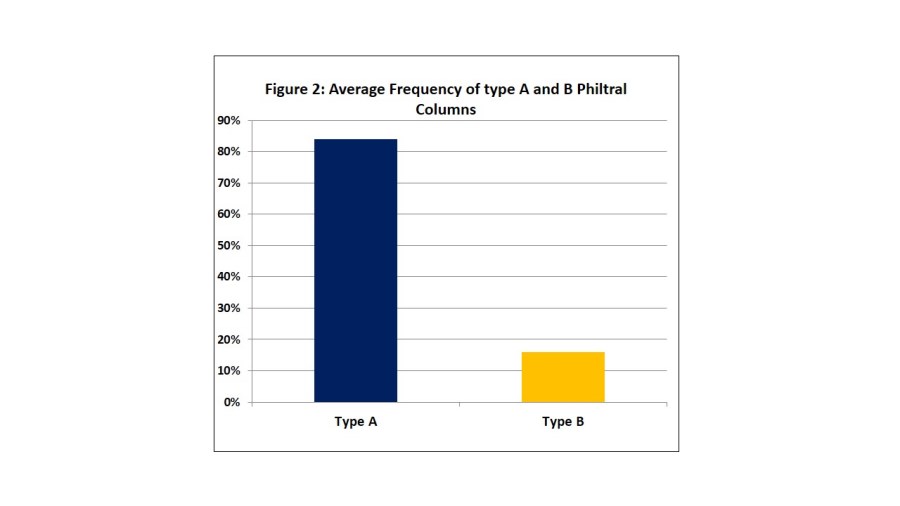
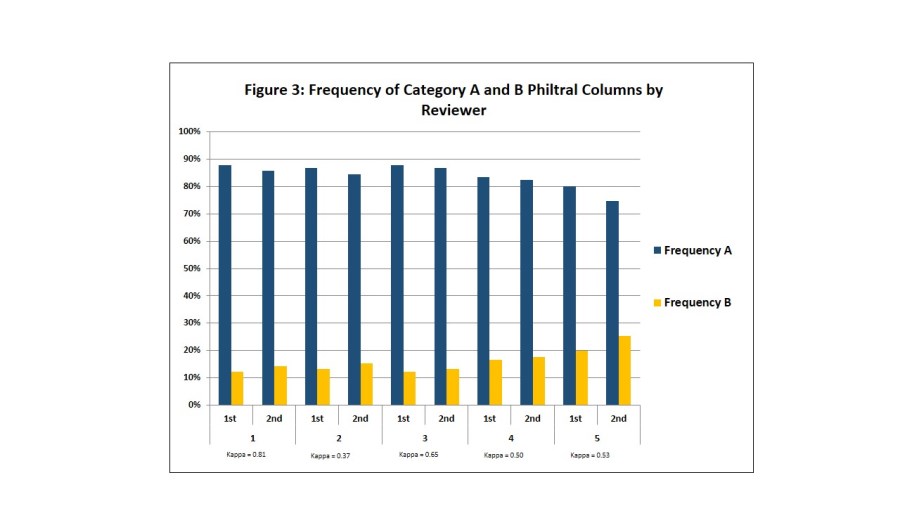
BACKGROUND: Traditional teaching is to perform a cleft lip repair that ideally places the surgical scar along the normal anatomic position of the philtral column. The rotation advancement is the most commonly performed technique for cleft lip repair and it places the surgical scar at the midpoint of the columella base. However, the position of the philtral column at the lip nose junction, relative to the columella, has never been clearly defined. It is unclear if current repair techniques adequately follow this principle. The goal of this study was to evaluate the location at which the normal philtral column arises relative to the columella at the lip nose junction. METHODS: Standardized photographs were taken of normal, unaltered philtral columns from healthy volunteers between the ages of 18 and 35. The location of the philtral column at the lip nose junction was then classified as type A) arising lateral to the base of the columella or type B) arising from the base of the columella (Figure 1). All images were evaluated by five reviewers at two separate times and intra and inter-rater reliability was then calculated. RESULTS: 91 Volunteers included 50 females (54.9%) and 41 males (45.1%). The average age was 27.6 (range 20 to 35). On average, 84% (range 75-88%) of participants were classified as type A compared to 16% (range 12-25%) classified as type B (p<0.0001)(Figure 2). This finding was true among all reviewers (Figure 3) with moderate intra-rater (Kappa=0.57) and inter-rater (kappa=0.48) agreement with at least 75% of photographs classified as type A. CONCLUSIONS: The majority of philtral columns did not arise from the columella and were classified as type A, arising lateral to the columella. In more than three quarters of individuals, there is a closer relationship to the lower lateral cartilage footplates. Current commonly performed cleft lip repair techniques that create a neo-philtral column at and sometimes across the base of the columella do not adequately restore the most frequent normal anatomic pattern. Cleft surgeons should keep in mind these normal anatomic relationships when designing lip repairs and use the non-cleft side philtral column as the most accurate and individualized template in unilateral repairs.
Back to 2014 Annual Meeting Posters
|




