|
|
|
|
|
Back to 2014 Annual Meeting Posters
Median Cleft Lip and Bifid Nose Deformity: Description, Classification and Treatment
Adam R. Kolker, MD1, John G. Meara, MD, DMD2, Alexander Sailon, MD1.
1Mount Sinai School of Medicine, New York, NY, USA, 2Children's Hospital, Boston, MA, USA.
BACKGROUND:
Median facial clefts are rare and challenging deformities caused by failure of fusion of the medial nasal prominences. These anomalies vary in severity, and may include microform lines or midline lip notching, incomplete or complete labial clefting, nasal bifidity, or severe craniofacial bony and soft tissue anomalies with orbital hypertelorism and frontoethmoidal encephaloceles. In this study, we present two cases, classify the spectrum of median cleft anomalies, and review our technical approaches to the surgical correction of median cleft lip and bifid nasal deformities. Embryology and associated anomalies are discussed.
METHODS:
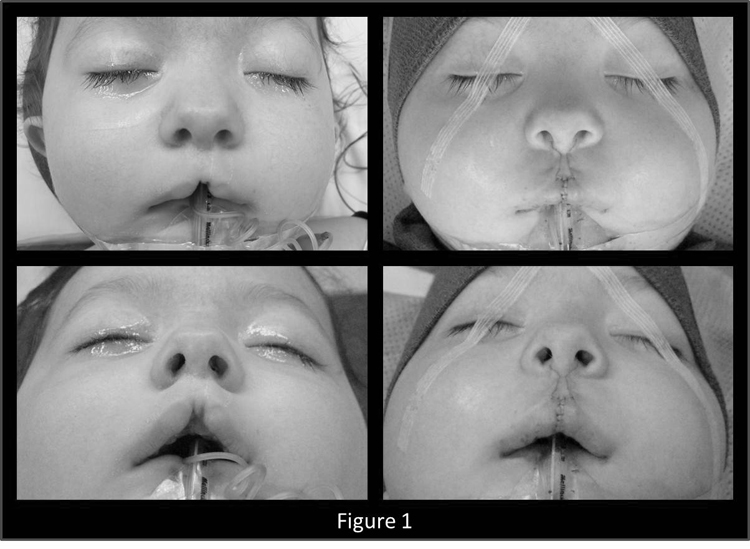
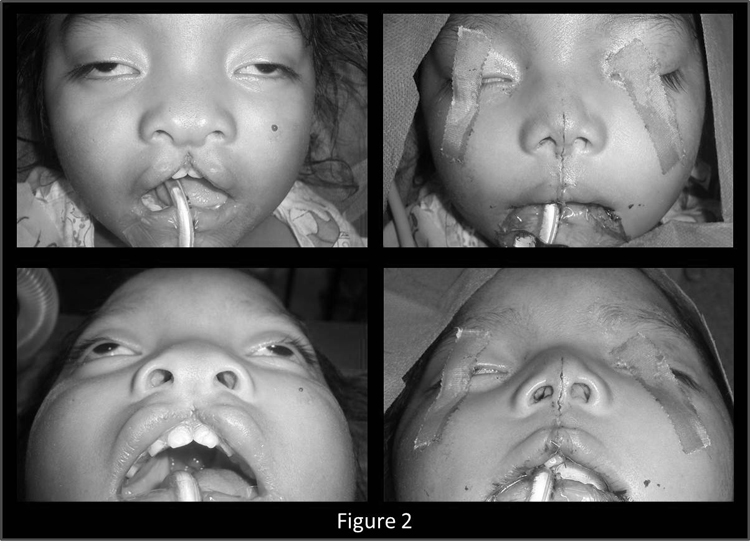
Our experiences with median incomplete cleft lip repair, and with median cleft lip and bifid nasal deformity treated with primary contiguous lip and nasal repair in one stage are described. Isolated median labial cleft repair is performed creating a prolabial flap with biconcave sides and a dart at its tip. Cupid’s bow peak-to-peak distance is 4mm with a collumela-labial junction base of 2mm. White roll-vermilion-mucosal flaps are incised. With no muscle continuity encountered beneath the prolabial flap, the orbicularis oris muscle bundles are dissected in each lateral lip complex in the subdermal and submucosal planes. After oral musosal repair, complete midline approximation of orbicularis pars marginalis and peripheralis is performed. Excess labial lateral element skin is excised into the nostril sill, and the philtral incisions are closed in layers. The lateral vermilion flaps are approximated to create a full tubercle (FIGURE 1). In one-stage median cleft lip and bifid nasal repair, the foreshortened lateral lip elements are elongated with convex curvilinear full thickness skin, orbicularis muscle, and mucosal parings. Vertical linear extensions are made onto the columella and nasal tip converging at the supratip. The medial crura of the lower lateral cartilages are dissected and the intervening redundant soft tissues excised. Bundles of m. orbicularis oris are dissected in each lateral lip complex, mucosa is approximated, and complete midline muscle repair is performed. Nasal cartilage is approximated to the midline, superfluous skin is excised, and vertical midline median tubercle, labial, and nasal closure is completed in layers (FIGURE 2).
RESULTS:
Functional and aesthetic anatomical correction was successfully achieved in each case without complication. A classification and treatment algorithm for the treatment of median cleft lip and bifid nose deformity is presented.
CONCLUSIONS:
The successful treatment of median cleft lip and bifid nose deformities first requires the identification and classification of the wide variety of anomalies. With exposure of abnormal nasolabial anatomy, the excision of redundant skin and soft tissue, anatomic approximation of cartilagenous elements, and complete orbicularis oris muscle repair, single-stage correction of median cleft lip and bifid nasal deformity can be safely and effectively achieved.
Back to 2014 Annual Meeting Posters
|
|




