
Use of A Pediatric Multi-Vector Mandibular Distractor for Treatment of Proximal Interphalangeal Joint Pilon Fractures
Rachel Pedreira, BA1, Brian H. Cho, MD2, Angela Geer, BS2, Ramon A. DeJesus, MD2.
1Johns Hopkins School of Medicine, Baltimore, MD, USA, 2Johns Hopkins University Department of Plastic and Reconstructive Surgery, Baltimore, MD, USA.
Background
Comminuted intra-articular fractures involving the PIP joint, or pilon fractures, present a therapeutic dilemma. Commonly, patients experience results that are less than ideal. Complications after healing include decreased range of motion, lack of articular symmetry, and possibly arthritis. In adults, external fixation with traction and early active range of motion (AROM)/passive range of motion (PROM) during healing is considered necessary for avoiding joint stiffness and attaining realignment. However, pediatric patients with pilon fractures present unique treatment considerations. Fractures in children may compromise growth plates and children are less compliant, however younger patients heal more quickly and may avoid joint stiffness. We present a unique approach to pediatric pilon fractures that employs open reduction and multi-vector external fixation with delayed AROM/PROM. In this setting, initial immobilization and significant traction allows for joint realignment and prevents non-compliance with staged distraction. We believe this immobilization lead to a superior outcome because, unlike adults, children tend to avoid stiffness and a larger distraction force allowed for sufficient joint realignment to regain ROM.
Methods
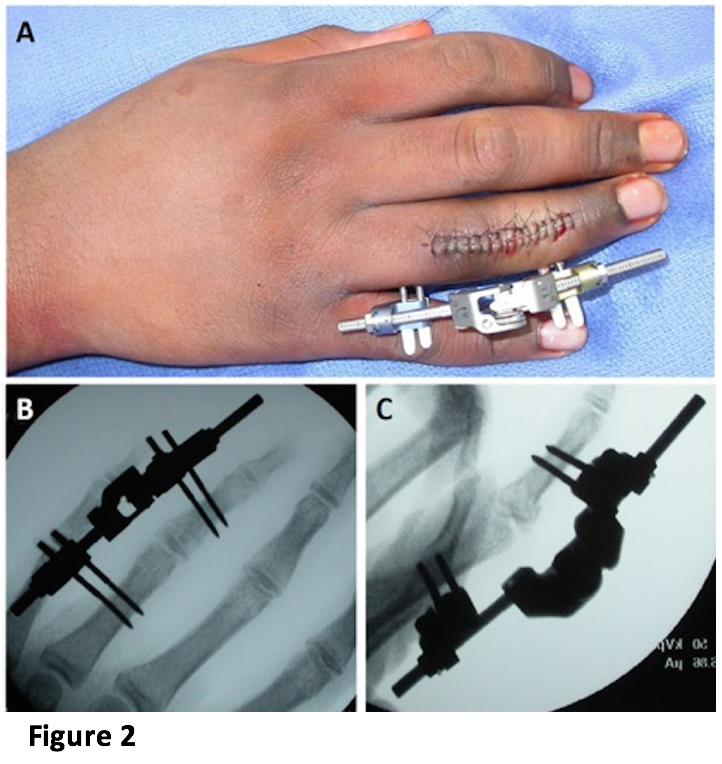
A right handed 13-year-old male sustained a right ring finger fracture and presented 12 days later. Radiographs revealed a comminuted Salter-Harris 4 fracture of the middle phalanx (Figure 1). The patient underwent open reduction and placement of multi-vector external fixation using a pediatric mandibular distractor/fixator. Significant traction was applied to distract the finger to length (Figure 2). 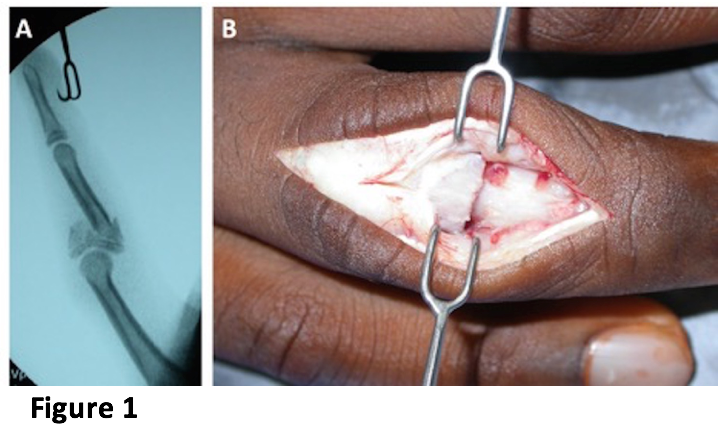
Results
Hardware was removed 6 weeks post-operatively and AROM was initiated after splinting. 8 weeks post-operatively, the patient started PROM. Strengthening was initiated 2 weeks later. ROM improved and rehabilitation was continued. 12 weeks post-operatively, the patient exhibited nearly equal grip strength. At 14 months follow up, radiographs showed complete healing and joint re-alignment. There was no deformity or pain and finger length was restored (Figure 3). 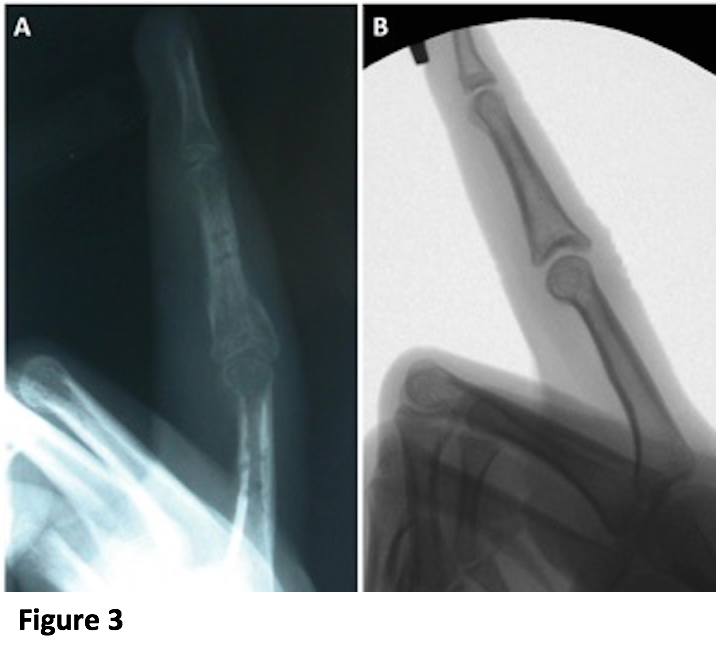
Conclusions
Management of pediatric pilon fractures is rarely described and presents unique considerations. Early stage traction and immobilization using a multi-vector mandibular fixator/distractor is suitable in a child because non-compliance is avoided and there is a decreased risk for stiffness. Combining early immobilization with subsequent staged AROM, PROM, and strengthening resulted in no loss of ROM and maintained articular symmetry.
Back to 2017 Program



