
Redefining the Rectus Sheath: implications for Abdominal Wall Repair
Imran R A Punekar, MD/PhD, Joseph S. Khouri, MD, Michael F. Catanzaro, BS, Aizaz L. Shaikh, MD, Howard N. Langstein, MD.
University of Rochester, Rochester, NY, USA.
BACKGROUND: The abdominal wall is frequently manipulated in a variety of reconstructive procedures, and its anatomy is well described. Our clinical observations, however, contradict the standard depiction of the components of the abdominal wall at various levels - particularly regarding the course of the transversus abdominis muscle (TA). Therefore, we sought to characterize the components of the rectus sheath at spinal levels L1-S1 in order to define key landmarks relevant to abdominal wall repair.
METHODS: We analyzed the abdominal CT studies of 100 healthy young (age 18-35, BMI 20-40) patients with suspected "renal calculi". Coordinates of key landmarks were recorded at each level with the aid of a specially-designed program which scaled all values and calculated distances between various points.
RESULTS: All subjects (41 male, mean BMI 26.4±4.81) had significant incorporation of the transversus abdominis within the rectus sheath (measured as the overlap between the abdominis rectus and transversus abdominis muscles) at L1 (4.20±1.16cm). 99% had TA incorporation within the rectus sheath at L2 (3.19±1.27cm), 86% at L3 (1.40±1.34cm), 36% at L4, and 2% at L5. Mean diastasis recti was significantly larger in males, not correlated to BMI, and greatest at L3-L4.
CONCLUSIONS: Our findings contradict classic teachings of abdominal wall structure and highlight the need for a cautious revisiting of the various permutations of component separation, particularly posterior component release. Furthermore, these anatomic landmarks may help predict the development or recurrence of ventral hernias, thus guiding patient selection and informing surgical technique. 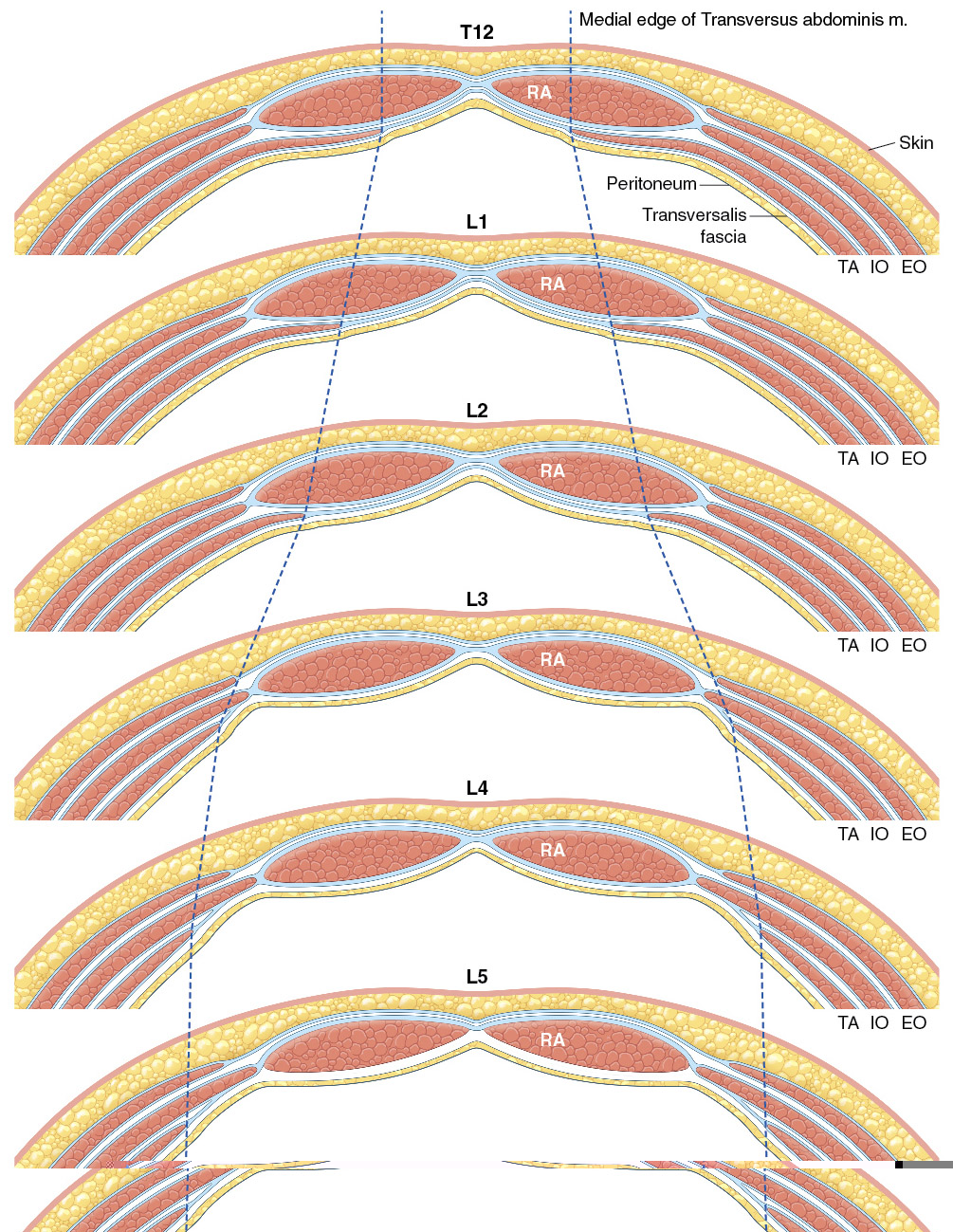
Back to 2017 Program



