
Minimal-Incision In Situ Cubital Tunnel Release: A New Technique and Review of the Literature
Brian H. Cho, MD1, Rachel Pedreira, BA1, Angela Geer, BS1, Michelle Seu, BA1, Ramon A. DeJesus, MD2.
1Johns Hopkins University, Baltimore, MD, USA, 2Bel Air Center for Plastic and Hand Surgery, Bel Air, MD, USA.
BACKGROUND: Cubital tunnel syndrome is one of the most common compression neuropathies of the upper extremity. In many cases, surgical intervention is required to adequately treat patients with cubital tunnel syndrome. Several surgical techniques have been described, including open and endoscopic in situ decompression, epicondylectomy, and nerve transposition. We present a novel minimal-incision technique for open in situ cubital tunnel release that provides effective nerve decompression while minimizing post-operative pain and discomfort. METHODS: We present a case example of a patient undergoing a minimal incision open in situ cubital tunnel release. Additionally, a pubmed search of all peer-reviewed studies from 1996 to 2016 reporting techniques and outcomes of the surgical management of cubital tunnel syndrome was performed. RESULTS: In situ cubital tunnel release may be performed using a 1.0-1.5 cm longitudinal incision positioned <0.5 cm posterior to the medial epicondyle (Fig. 1A). With careful retraction, longitudinal spreads with tenotomy scissors performed down to the roof of the cubital tunnel avoiding the medial antebrachial cutaneous (MABC) nerve (Fig. 1B). Blunt dissection with the Langenbech miniature retractors is performed proximal at the anatomical plane of the intermuscular septum and distally over the flexor pronator aponeurosis. Two miniature retractors are placed proximally at the developed plane at approximately 30 degrees from the longitudinal axis of the incision. The operating room table is then raised to eye level to optimize visualization during the in situ release. A longitudinal cut is made at the roof of the cubital canal creating a window to visualize the nerve. Under direct visualization, the ligament is retracted with the forceps and the tenotomy scissors are oriented proximal and the medial intermuscular septum is released for approximately 5 cm proximal (Fig. 1C). Similarly, the ligament of Osborne and the fascia of flexor carpi ulnaris are released under direct visualization. The incision is closed with buried absorbable suture (Fig. 1D). CONCLUSIONS:
Current minimally invasive techniques have gained popularity due to the decrease in operative morbidity, complications, and healthcare costs. Current methods for cubital tunnel release often involve the use of laparoscopic instruments or large open incisions. We present a minimal-incision in situ cubital tunnel technique that utilizes an incision less than 1.5cm while providing adequate exposure for complete nerve decompression. Further studies are necessary to compare the clinical the outcomes of patients undergoing minimally invasive cubital tunnel release procedures.
Figure 1. Minimal-incision in situ cubital tunnel release. 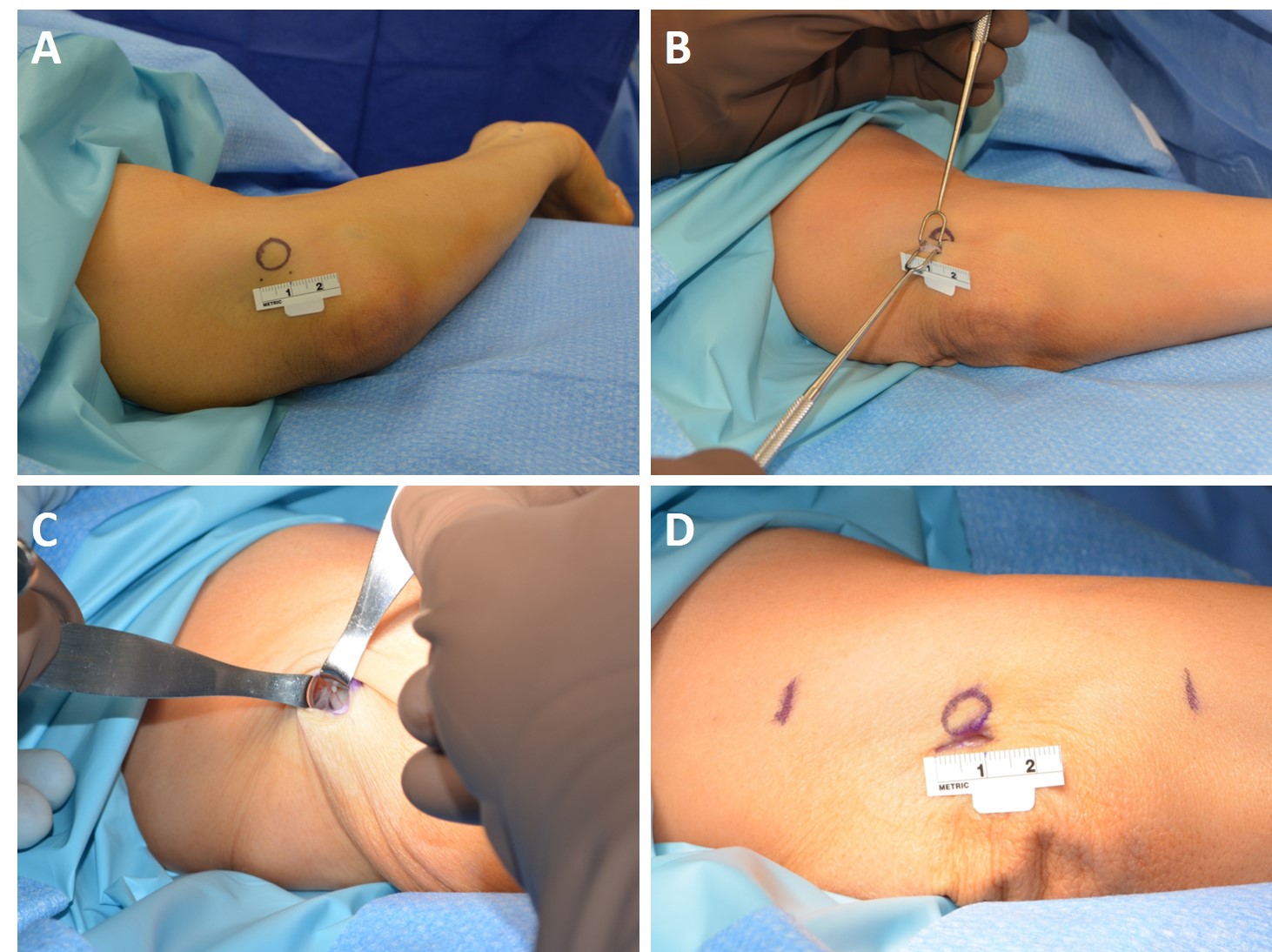
Back to 2017 Program



