
A quantitative analysis of weight gain following mandibular distraction osteogenesis
Cyril S. Gary, Sharon Marczewski, Patricia M. Vitagliano, Derek M. Steinbacher.
Yale School of Medicine, New Haven, CT, USA.
Background
Infants with microretrognathia suffer from upper airway obstruction, which leads to difficulties with both breathing and feeding. Mandibular distraction osteogenesis (MDO) represents one therapeutic option designed to maximally open the airway in such patients. MDO is expected to improve breathing, but should also positively impact feeding. We hypothesize that feeding and weight gain will improve significantly following MDO.
Methods
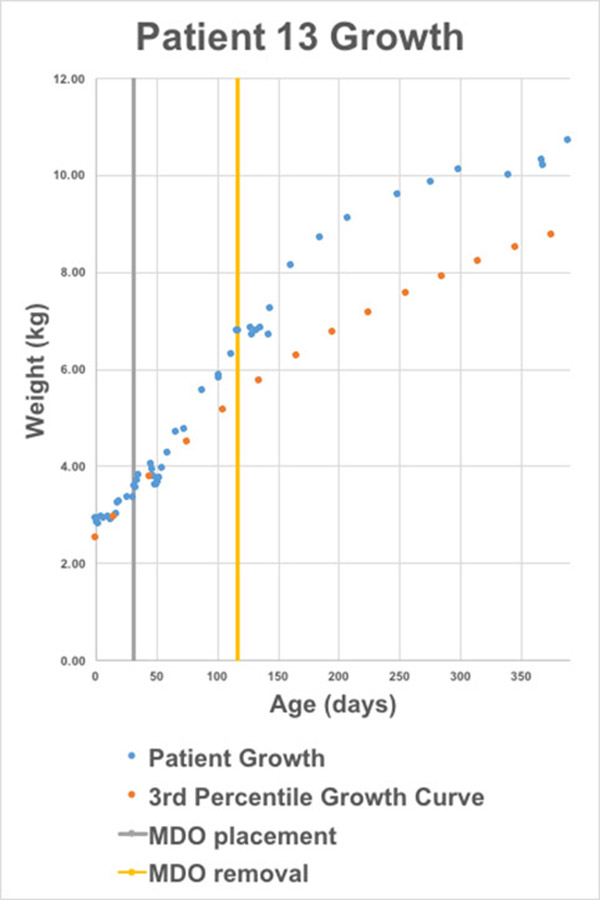
This retrospective chart review quantitatively assessed feeding and weight gain for 22 microretrognathic infants (12 boys, 10 girls) before and after MDO. Demographic, diagnostic, perioperative, and distraction protocol data was collected, along with weights at available time points. Each patient's weight plotted over time was then compared to his or her closest percentile growth curve as reported by the World Health Organization (WHO; Fig. 1). Linear regression analysis was utilized in several time intervals before and after surgical intervention, and the slope of each fitted line was then used to calculate both the actual average daily weight gain (ADWG) for each infant and expected ADWG for each infant's respective growth curve. Percentiles were calculated from weights using published WHO data. Actual vs. expected weight gains, along with percentiles, were compared using a Wilcoxon matched-pairs signed rank test.
Results
We found significantly lower weight gain than expected from birth to time of MDO, and significantly greater weight gain than expected for three time intervals following surgical intervention (Table 1; all values reported as mean and (standard error of mean)). Average growth percentiles similarly decreased from birth to MDO and increased after MDO, and were calculated to be as follows: at birth = 35.6 (6.7), at MDO placement = 21.4 (6.2), at MDO removal = 28.0 (6.7), and at 6 months after MDO = 33.1 (6.9). The decrease in average growth percentile from birth to MDO placement (p = .0060), and the increase from MDO to removal (p = .0412) and from MDO to 6 months post-operatively (p = .0053) were statistically significant.
Table 1 – expected vs. actual ADWG for infants treated with MDO
| Birth to MDO | MDO to device removal | MDO to 6 months post-operatively | MDO to 12 months post-operatively | |
| Actual ADWG, g/day | 17.2 (2.3) | 22.8 (2.3) | 20.1 (1.7) | 16.5 (1.3) |
| Expected ADWG, g/day | 26.1 (1.0) | 18.7 (1.4) | 16.5 (1.2) | 13.4 (1.0) |
| Difference, g/day | -8.9 | +4.1 | +3.6 | +3.1 |
| p-values | .0014 | .0194 | .0065 | .0069 |
Conclusion
MDO results in significant weight gain following operative intervention. MDO is an effective modality not just for the treatment of airway obstruction but also for problems with weight gain in microretrognathic infants.
Back to 2017 Program



