
Photochemical Tissue Passivation (PTP) Prevents Contracture of Full Thickness Wounds
Rachel L. Goldstein, D.O.1, Gem Runyan, M.S.1, Mark A. Randolph, M.A.S.1, Michael C. McCormack, M.B.A.1, Martin C. Mihm, Jr., M.D.2, Robert W. Redmond, PhD1, William G. Austen, Jr., M.D.1.
1Massachusetts General Hospital, Boston, MA, USA, 2Brigham and Women's Hospital, Boston, MA, USA.
BACKGROUND: Large surface area wounds, from burns, trauma, or iatrogenic injury, often result in significant scarring and wound contracture. Despite treatment with current therapies, contracture can still develop as a product of myofibroblast activity during the process of normal wound healing. Photochemical Tissue Passivation (PTP), an established, safe, and user-friendly treatment modality, induces extracellular collagen cross-linking and limits myofibroblast activity in healing wounds. We hypothesized that PTP treatment of wounds would reinforce the wound bed with cross-linked collagen, blunt the fibrotic response, and thereby limit contracture and associated morbidities.
METHODS: Full-thickness, excisional 1cm x 1cm wounds were created on the dorsal surface of thirty-two C57BL/6 mice. The native skin around the wound perimeter was tattooed with a 30-gauge hypodermic needle. Wounds in the control group (n=16) were untreated. Treated wounds (n=16) received PTP immediately after wound creation with application of 0.1% solution of Rose Bengal (RB), a photosensitizing dye, and exposure to 60J/cm2 of green light (λ = 532nm). Wounds were serially photographed over six weeks to measure the area within the tattoo perimeter. Percent contracture was calculated by dividing the tattoo area at each timepoint by its initial area. At 7, 14, 21, and 42 days after wound creation, mice were euthanized and wound skin was harvested for histology. Specimens were stained with H&E and Masson's Trichrome, and reviewed by a dermatopathologist.
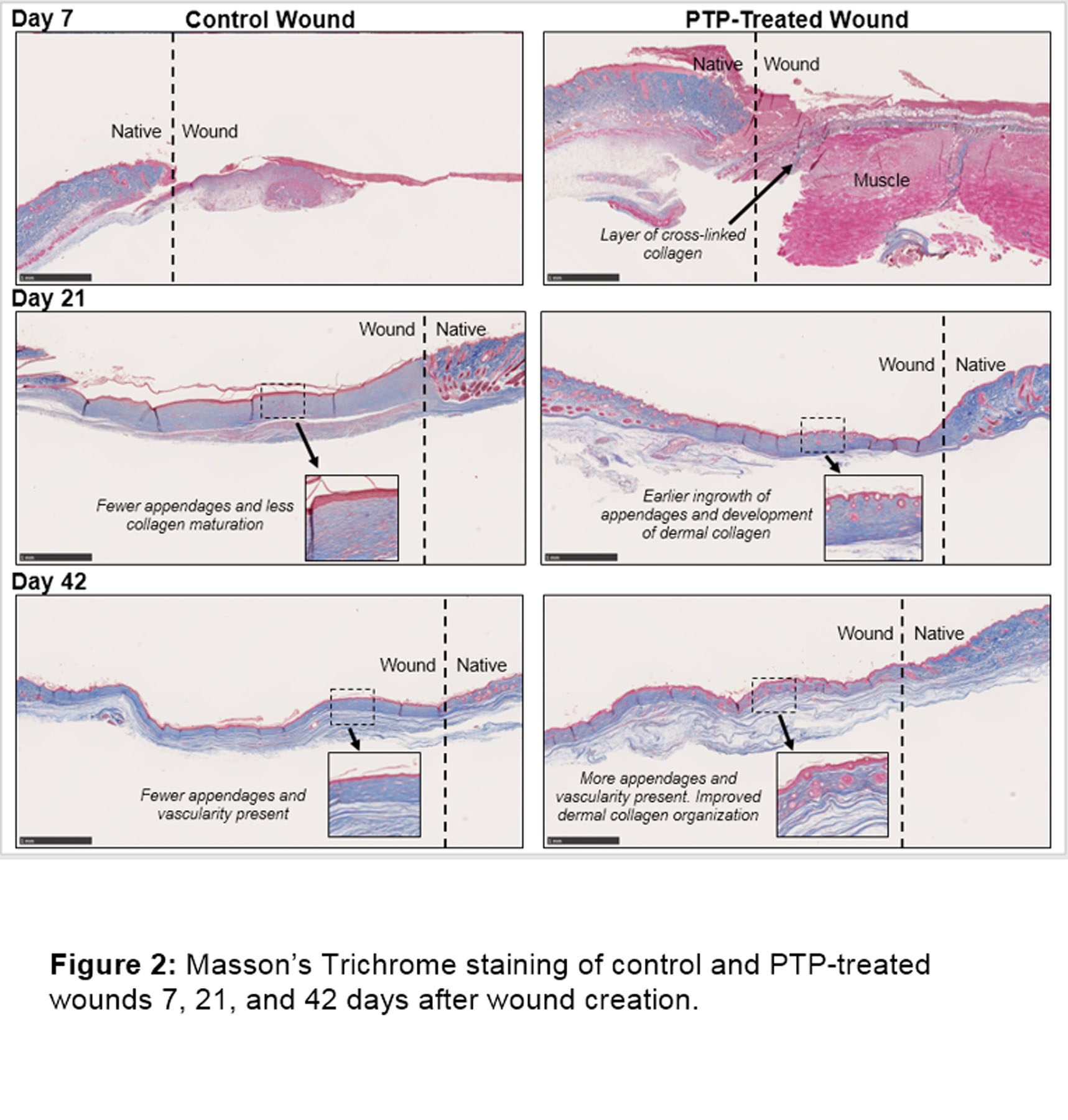
RESULTS: All wounds grossly epithelialized the first week and were fully healed by the end of the study. Treated wounds contracted significantly less than controls for the length of the study (Figure 1). Control wounds exhibited almost 20% more contracture by Day 7 (67.1±17.1% vs 80.3±8.5%; p=0.014, n=16/group), and over 80% more by Day 14 (27.8±8.6% vs 50.3±11.9%, p<0.05, n=12/group). Degree of contracture plateaued for both groups by Week 3, with 1.05-fold less contracture in treated wounds on Day 21 (p<0.05, n=8/group). By Day 42, wounds had contracted to 13.6±5.6% in controls and 35.2±2.9% in treated wounds, a 1.59-fold difference (p=0.003). On histologic review, PTP promoted ingrowth and development of dermal collagen in the wound, which organized to mimic native skin to a substantially greater degree than in control wounds. PTP also promoted neovascularization and development of skin appendages, earlier and to a greater degree, compared to control wounds (Figure 2).
CONCLUSIONS: PTP significantly limits contracture of full-thickness wounds, and accelerates and improves wound healing. Wounds treated with PTP histologically demonstrate more mature structural organization than untreated wounds, and closely resemble native skin. PTP treatment may be applicable not only for excisional wounds, but also for wounds with a high incidence of contracture and associated morbidity, including burns, skin grafts, and traumatic injuries. 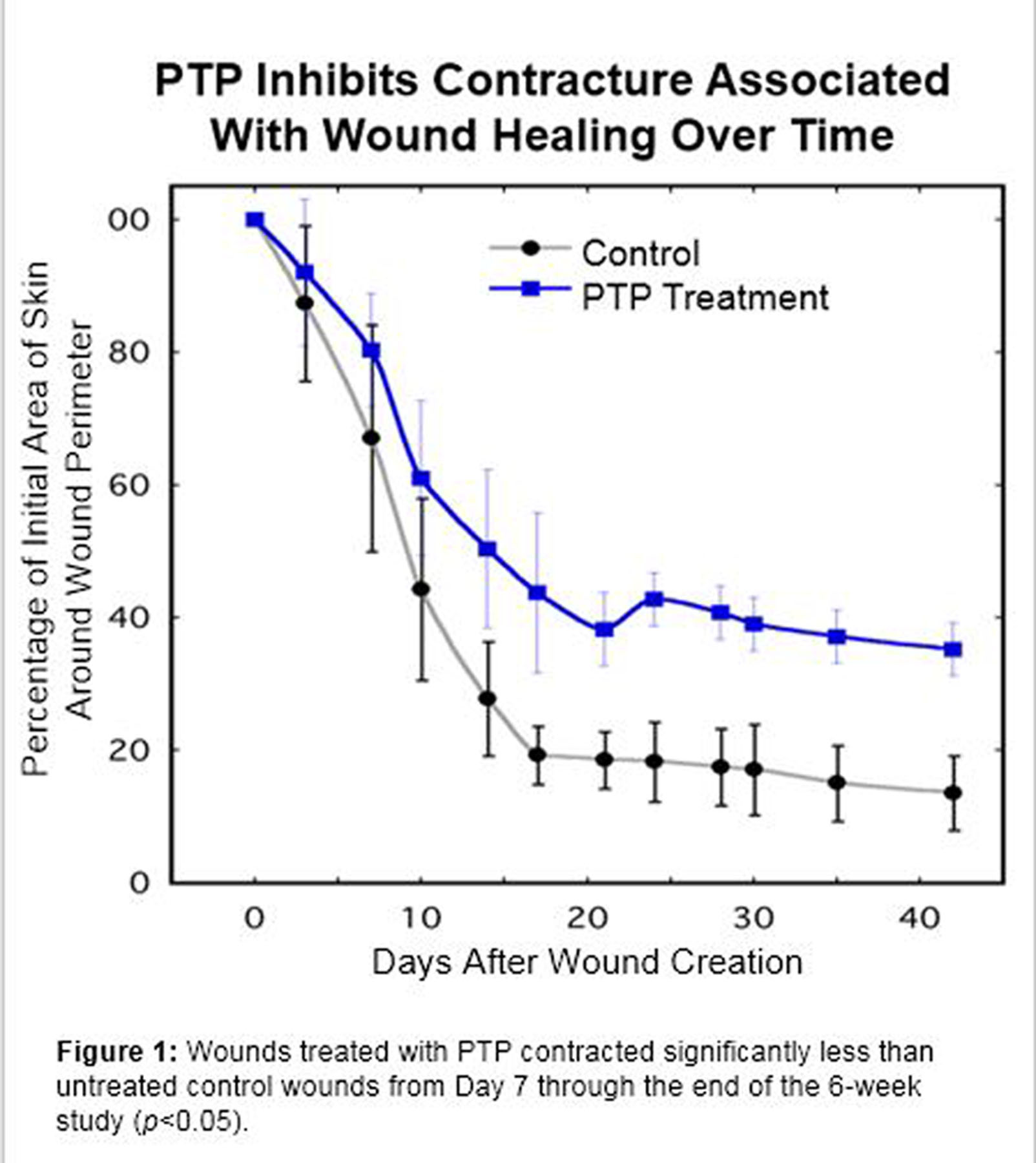
Back to 2017 Program



