
A Study of 39,476 Firearm Injuries in the Pediatric Population: Trends and Disparities in Flap Reconstruction
Austin D. Chen1, Klaas Ultee, PhD2, Alexandra Bucknor, MBBS, MRCS, MSc1, Anmol S. Chattha, BA1, Patrick P. Bletsis, BSc1, Salim Afshar, MD, DMD3, Bernard T. Lee, MD, MBA, MPH, FACS1, Samuel J. Lin, MD, MBA, FACS1.
1Beth Israel Deaconess Medical Center, Boston, MA, USA, 2Erasmus University, Rotterdam, Netherlands, 3Boston Children's Hospital, Boston, MA, USA.
BACKGROUND:
Firearm injuries in children and adolescents have been examined nationally, however, there has been little analysis of regional trends or treatment modalities. Plastic surgeons have a unique role in reconstruction of firearm-related defects. We investigated national and regional trends of firearm injuries and flap reconstruction.
METHODS:
A retrospective analysis of the Healthcare Cost and Utilization Project Kids' Inpatient Database for the years 2000, 2003, 2006, 2009 and 2012 was carried out. Data for patients ≤20 years admitted with firearm injuries were retrieved. The Cochran-Armitage test was used to evaluate national and regional trends in firearm injury incidence and flap reconstruction over time. Patient characteristics, injuries and outcomes were analyzed for non-flap reconstruction (NFR) and flap reconstruction (FR).
RESULTS:
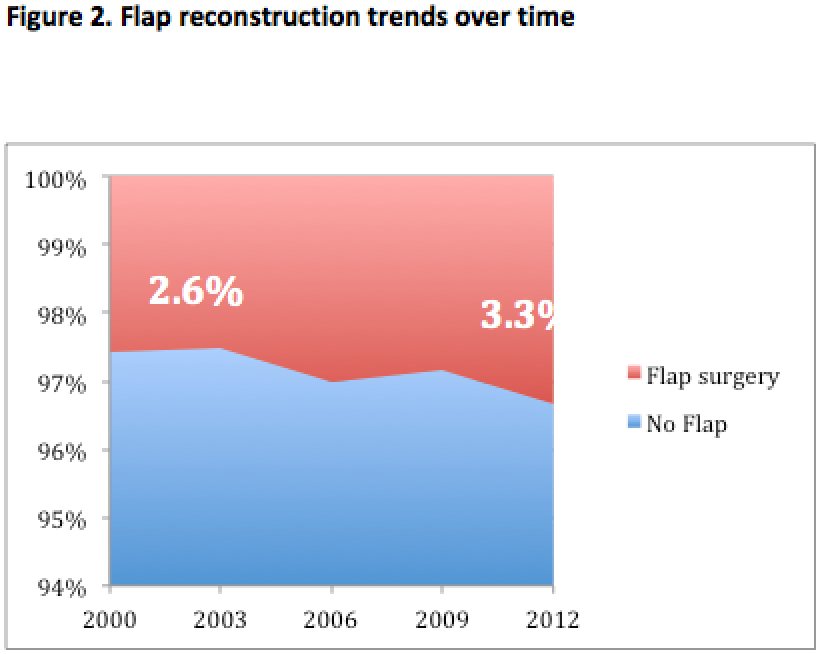
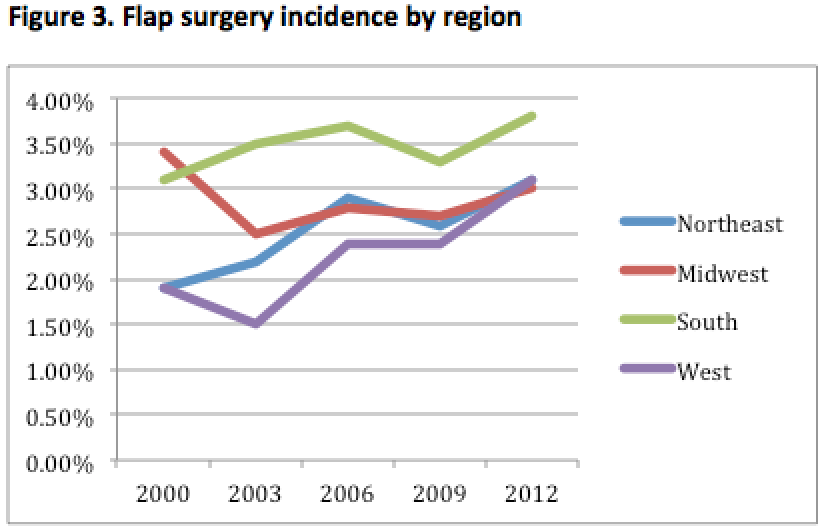
There were 39,476 pediatric patients admitted for firearm injuries over the study period. There was no change in incidence per one million population (from 111 per million in 2000 to 92 per million in 2012, see figure 1). Flap reconstruction has increased (2.57% to 3.34%, p=0.003)(figure 2). Northeast and West regions both show a significant increase in FR from 1.90% to 3.10% (p=0.034 and p=0.004, respectively)(figure 3). There were more male FR patients compared to NFR patients (92.3% vs. 89.9%, p=0.009). There were significant differences in ethnicity (p<0.001), insurance (p<0.001), and income (p<0.001). Patients not receiving flap reconstruction were more often of African American (55.6% vs. 51.2%) or Hispanic (22.5% vs. 15.4%) ethnicity, in the first quartile of income (47.8% vs. 44.0%) or self-pay (21.3% vs. 16.3%) or no charge (1.5% vs. 0.6%). There were significant differences in hospital size (p<0.001), teaching status (p<0.001) and region (p<0.001). Patients not receiving flap reconstruction were more often admitted at small (6.1% vs. 3.6%) or medium (22.2% vs. 19.5%), rural (2.8% vs. 2.1%) or urban non-teaching (15.3% vs. 10.2%) centers in the Northeast (16.4% vs. 14.6%) or West (26.8% vs. 20.6%). Patients with FR had significantly more infections (4.7% vs. 1.1%, p<0.001), respiratory complications (10.5% vs. 8.1%, p=0.004), wound dehiscence (0.6% vs. 0.4%, p<0.001) and acute renal failure (2.7% vs. 0.7%, p<0.001). A significantly greater number of NFR patients had concomitant injuries (p<0.001).
CONCLUSIONS:
Plastic surgeons have an important role in the management of pediatric firearm injuries is an important aspect of plastic surgery, as evidenced by the increase in flap reconstruction over time. However, there are geographical and patient-level disparities in the receipt of flap reconstruction and further research may aim to understand the reasons for this. 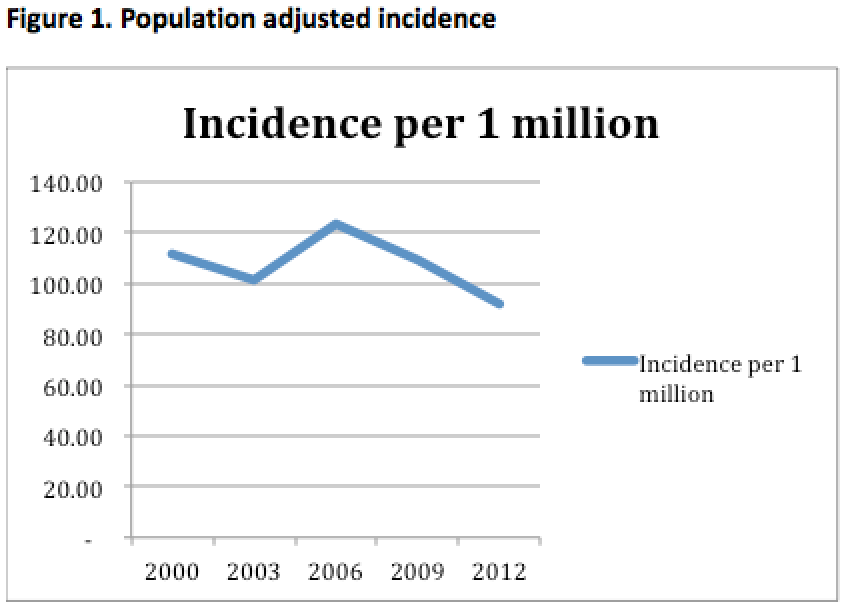
Back to 2017 Program



