
Putting a price on aesthetics in breast reconstruction after nipple-sparing mastectomy: A cost-minimization analysis of skin banking with deep inferior epigastric perforator flaps
Andrew L. Weinstein, MD, MS, Rachel Akintayo, MD, David M. Otterburn, MD.
New York Presbyterian / Weill Cornell Medicine, New York, NY, USA.
BACKGROUND: Breast skin necrosis after nipple-sparing mastectomy (NSM) and deep inferior epigastric perforator (DIEP) flap reconstruction substantially impacts cosmetic outcome and patient satisfaction. While debridement and primary closure may be used to treat small areas of skin necrosis, similar management of larger areas results in breast contour abnormalities and nipple malposition. Skin grafting might mitigate these sequelae, but creates a color and texture mismatch with native breast skin. In contrast, abdominal skin on the DIEP flap is an excellent match and can be banked beneath mastectomy skin to reconstruct large areas of necrosis with optimal aesthetics. The purpose of this study was to determine the cost of skin banking with DIEP flaps compared to that of managing skin necrosis with alternative modalities.
METHODS: A retrospective review of all patients who underwent breast reconstruction with DIEP flaps by the senior author at Weill Cornell Medicine between 2011 and 2014 was conducted to identify the incidence and surface area of full-thickness skin necrosis after NSM as well as nipple-areola complex (NAC) pathology on permanent section requiring excision. Current Procedural Terminology codes for complex closure, split-thickness skin graft, application of skin substitute, full-thickness skin graft (FTSG), and revision of reconstructed breast were determined and corresponding Medicare reimbursement costs were calculated. Cost-minimization and sensitivity analyses were performed using TreeAge Pro version 2017 (TreeAge Software, Inc., Williamstown, MA).
RESULTS: 68 breasts in 38 patients underwent NSM and DIEP flap breast reconstruction. The incidence of breast skin necrosis was 10.3% overall, 1.5% <10cm2 and 8.8% >10cm2, and averaged 58.3cm2 (median 36 cm2). In 2.9% of cases, permanent pathology required excision of NAC. The average per patient cost of skin banking with DIEP flaps was $1,224.44, and as follows for the management of skin necrosis without banked skin: $380.90 for STSG alone; $804.80 for STSG and skin substitute; and $385.43 for FTSG. Based on the sensitivity analysis, the cost of skin banking was less than that of managing skin necrosis with STSG and skin substitute when the incidence of necrosis >10cm2 exceeded 25.3% (Figure).
CONCLUSIONS: Although the average per patient cost of skin banking may be higher than that of managing skin necrosis without banked skin, the cost differentials between techniques examined are relatively low. Given that the use of banked skin to reconstruct areas of skin necrosis yields optimal aesthetics, we therefore recommend preemptive skin banking in breast reconstruction with DIEP flaps. 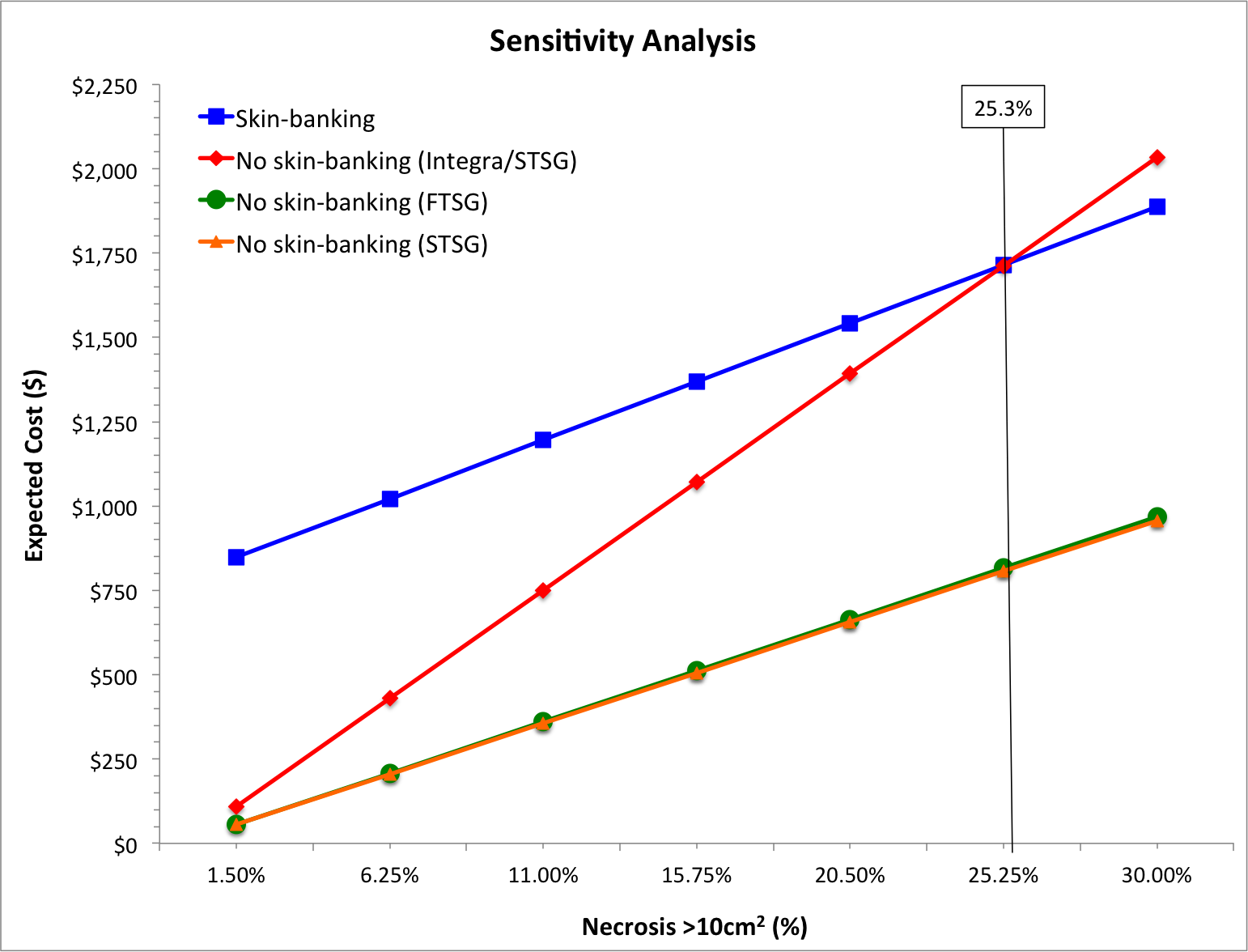
Back to 2017 Program



