
Epinephrine and the Traumatic Hand in the Emergency Room (ETHER study)
Angela T. Prescott, MD1, Benjamin K. Schilling, MS2, Jignesh V. Unadkat, MD1.
1University of Pittsburgh Medical Center, Pittsburgh, PA, USA, 2University of Pittsburgh, Pittsburgh, PA, USA.
BACKGROUND: The myth forbidding the use of lidocaine with epinephrine in the hand has been debunked. Prior studies demonstrate that it is safe to use epinephrine in digital blocks, carpal tunnel surgery, and elective hand procedures under the "Wide Awake Local Anesthetic with No Tourniquet" (WALANT) methodology. Now we challenge the dogma in the setting of acute traumatic hand injuries. Our hypothesis is that outcomes and complication rates (infection, necrosis, stiffness, re-operation) are not statistically different between patients who are treated with lidocaine plain versus those treated with lidocaine with epinephrine.
METHODS: With IRB approval, we performed a retrospective chart review of patients presenting to the UPMC emergency department with a diagnosis of acute hand trauma from July to September 2018. Thirty-eight patients with 58 injuries met inclusion criteria and were stratified into two groups: those who were treated using 1% lidocaine with epinephrine versus those with 1% lidocaine plain. Patients under 18 years old, and those with inadequate follow up were excluded. Primary endpoints included infection, need for antibiotics, necrosis, stiffness, and need for re-operation. Secondary endpoints included the need for occupational therapy (OT), length of OT, and time to final clinic visit (or resolution of injury). Fischer’s exact test, anova one-way, and multiple fit models were used for statistical analysis.
RESULTS: Patient cohorts were evenly matched in terms of demographics, co-morbidities, and mechanism of injury. The use of epinephrine in patients with acute hand trauma had no statistical correlation with increase rates of infection (p=1.0), need for antibiotics (p=0.77), stiffness (p=1.0), necrosis (p=1.0), or re-operation (p=1.0). Use of epinephrine was not associated with increased need for OT (p=1.0), length of OT (p=0.4), or time to resolution of issue (p=0.5). Post-injury infection was significantly associated with patient comorbidity and mechanism of injury (p=0.007), not type of anesthetic used (p=1.0). Need for repeat antibiotics was significantly correlated with patient comorbidities and smoking status (p=0.003), not type of anesthetic (p=0.49). Similarly, stiffness and re-operation rates were related to patient comorbidities (p=0.002) and not type of anesthetic used (p=1.0).
CONCLUSIONS:
Our early data demonstrates that practitioners of hand surgery may continue to use lidocaine with epinephrine in patients with acute traumatic hand injuries without posing further increased risk of post-traumatic complications. 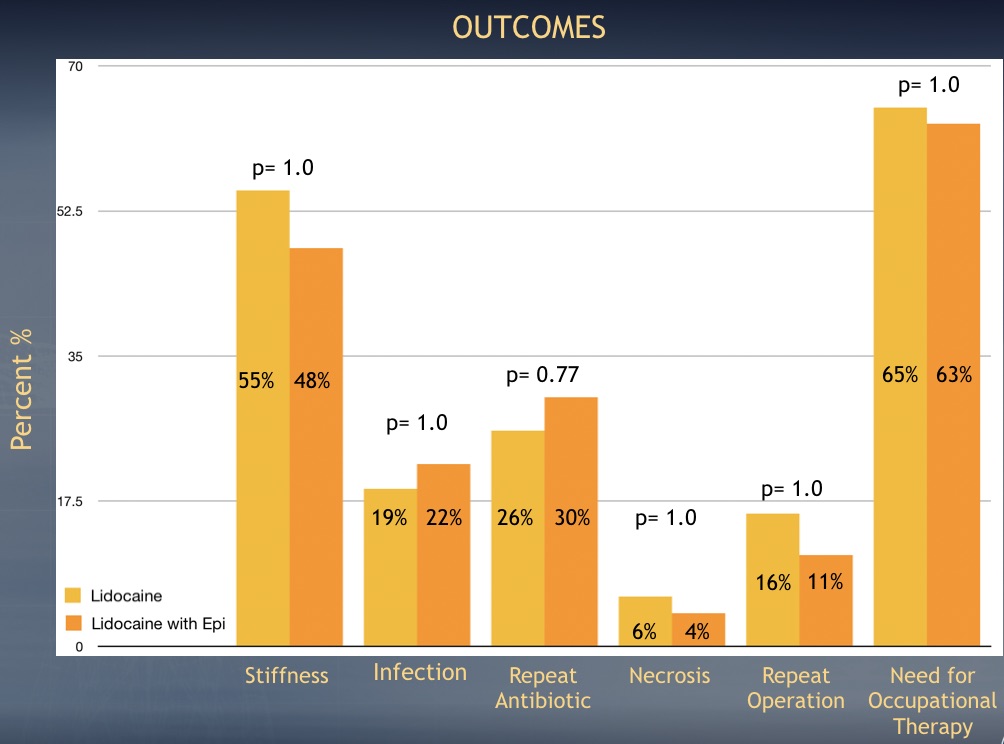
Back to 2019 Abstracts