
Make your own DIEP: Perforator Delay Improves DIEP flap reliability
suhail kanchwala.
university of pennsylvania, merion, PA, USA.
Background:
We have applied the delay phenomenon to Deep Inferior Epigastric Perforator (DIEP)DIEP flap reconstruction in order to 1) reliably harvest single vessel DIEP flaps without congestion 2) minimize abdominal wall morbidity, and 3) maximize aesthetics.
Methods:
At first stage,At the first stage mastectomy and prepectoral tissue expander placement occurs is performed with an abdominal perforator delay. Selection criteria for the index We select a perforator is thewith a shortest intramuscular course with a and low central location to minimize myofascial insult and to maximize a low scar placement. All Other other perforators are ligated including thealong with the SIEA/V vessels and the incisions are closed. The flaps are transferred to the chest to complete reconstruction in a delayed fashionreconstruction is then completed after a 2 week delay period. Any mastectomy skin flap necrosis is debrided prior to final flap inset minimizing postoperative wounds.
Results:
Eight-five patients underwent 128 single perforator DIEP flaps. Mean age and BMI was 50.9 years and 29.1 kg/m2. Mean time between stages was 18.1 days. Two perforator complications occurred with 2 flap losses. Length of stay following flap transfer was 2.2 days. 65.9% of patients avoided narcotics entirely. Operative breast complications included arterial thrombosis (0.8%), venous congestion (1.6%), and fat necrosis (1.6%). Operative abdominal complications included dehiscence (5.6%), seroma (2.4%), and skin flap necrosis (1.2%).
Conclusions:
The two-stage delayed DIEP flap technique allows for selection of the ideal perforator based on location and course. This flexibility permits less dissection, less pain, and better scar location. Perforator delay mitigates the trade-off of blood supply and morbidity in free flap breast reconstruction.
Figures:
Figure 1: 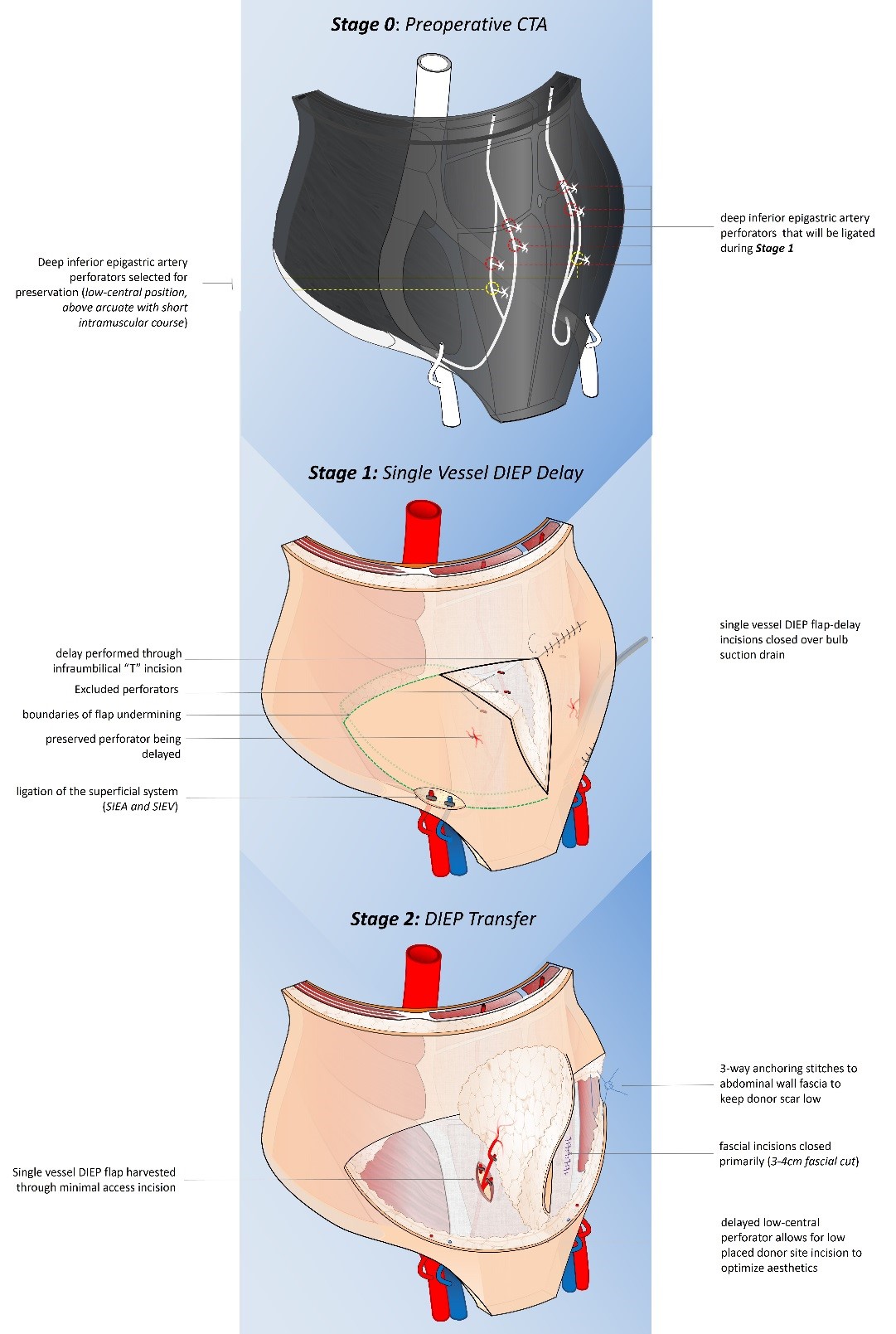
Back to 2019 Abstracts