
A Post-Operative Protocol for Autologous Free Flap Breast Reconstruction Optimizing Resources and Patient Safety
Darya Fadavi, BS, Allison Haley, BS, Nima Khavanin, MD, Franca Kraenzlin, MD, Tobias J. Bos, BSc, Brian H. Cho, MD, Hannah M. Carl, BS, Deepa Bhat, MD, Benjamin T. Ostrander, BS, Michele A. Manahan, MD, Gedge D. Rosson, MD, Justin M. Sacks, MD, MBA, FACS.
Johns Hopkins School of Medicine, Department of Plastic and Reconstructive Surgery, Baltimore, MD, USA.
BACKGROUND: The increase in popularity of using deep inferior epigastric artery perforator (DIEP) flaps for breast reconstruction creates an opportunity for standardization of post-operative patient care. At some institutions and practices, current standard of care involves admission to monitored beds and the Intensive Care Unit (ICU) for up to 72 hours post-operatively with subjective monitoring to assess for flap compromise. At our institution, we have implemented a post-operative pathway involving flap monitoring using near infrared spectroscopy (NIRS) devices to objectively assess capillary perfusion, without any admission to the ICU (Figure 1). This study serves to assess the outcomes of this post-operative pathway and determine its feasibility as an alternative to current practices. METHODS: This study comprised a retrospective cohort of 153 patients and a total of 239 DIEP flaps at our institution from January 2013 to August 2014. Data of interest included patient demographics and medical history as well as complication rates and date of hospital discharge. Data gathered was then compared to published rates in the literature. Institutional costs were collected and compared to the theoretical cost of a 24 hour post-operative ICU stay.
RESULTS: The average patient age in our study was 50 years (SD=10.2) with an average BMI of 29.4 kg/m2 (SD=5.2). Overall, the flap failure rate was 1.3%, and reoperation rate 3.9%, which were comparable to published rates in the literature. 71% of patients were successfully discharged by post-operative day 3, and nine patients were discharged past post-operative day 5. The theoretical cost saving difference between patients on the surgical floor and on the ICU was found to be $1,053.
CONCLUSIONS: Our pathway involving continuous tissue oximetry using a NIRS device and flap checks on the surgical floor resulted in acceptably low flap failure and reoperation rates that were comparable to those published in the literature. Our median discharge on post-operative day 3 is among the earliest in the literature, and allows for a decreased risk of nosocomial infection and cost. Monitoring of our DIEP patients on the surgical floor also avoids using the scarce hospital resource of ICU beds. Our post-operative DIEP pathway is a viable and safe alternative to the current practice of ICU-based patient care. Non-utilization of ICU beds in tertiary facilities for breast free flap patients allows efficient allocation of resources while not compromising patient outcomes. 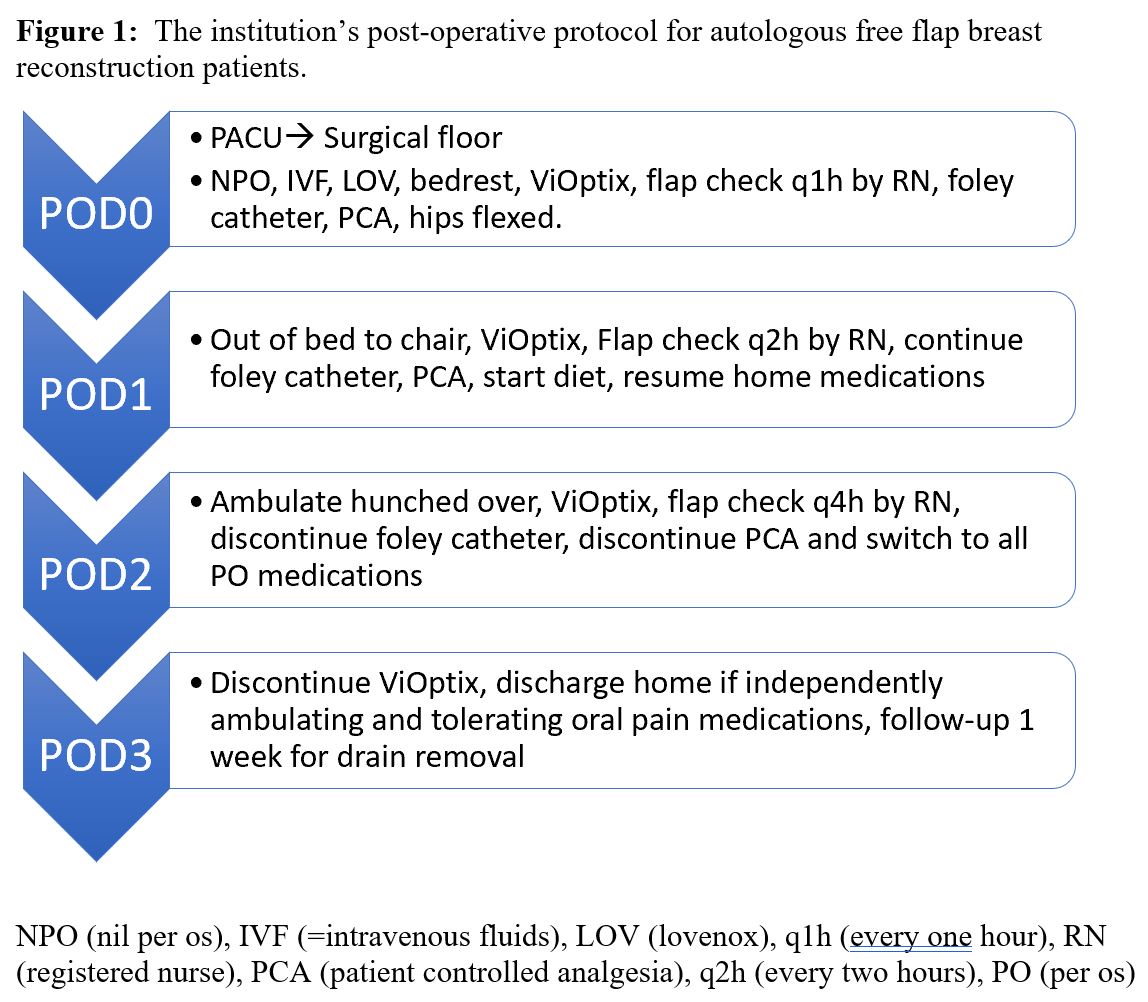
Back to 2019 Abstracts