
Ischemic complications after nipple-sparing mastectomy: predictors of reconstructive failure in implant-based reconstruction and implications for decision-making.
Jonathan M. Bekisz, MD, MSci, Ara A. Salibian, MD, Jordan D. Frey, MD, Mihye Choi, MD, Nolan S. Karp, MD.
NYU Langone Health, New York, NY, USA.
Purpose: The sequelae of mastectomy skin flap and nipple-areolar complex ischemia can be devastating complications in immediate reconstruction after nipple-sparing mastectomy (NSM). While risk factors for ischemic complications are well known, predictors of reconstructive failure with major skin envelope ischemia and implications for decision-making remain to be fully elucidated.
Methods: A retrospective review was performed of all cases of NSM and immediate implant-based reconstruction at a single institution from 2006 to June 2018. All cases with major ischemic complications, defined as either mastectomy flap necrosis or nipple-areolar complex (NAC) necrosis requirement debridement were included. Data on patient demographics, mastectomy and reconstruction characteristics, additional reconstructive complications and the nature and management of ischemic complications were collected and analyzed. Cases requiring explantation or implant exchange were compared.
Results: Out of 1,345 cases of NSM, 70 (5.2%) had major ischemic complications. Most were two-stage tissue expander reconstruction (74.3%) with ADM used in 50% of cases and mesh in 7.1%. Average mastectomy weight was 645.7 grams.
63 cases (90%) had major mastectomy flap necrosis, 18 (25.7%) had full NAC necrosis and 11 (15.7%) had both. 5 cases (7.1%) underwent implant exchange at the time of debridement and 15 cases (21.4%) required explantation and delayed reconstruction with two-staged implant-based (9 cases), latissimus dorsi and implant (4 cases) and autologous (2 cases) reconstruction. Debridement of necrosis was performed at an average of 27.8 days after reconstruction with an average debridement size of 27.8 cm2.
Cases that required explantation had a significantly lower BMI (22.3 versus 24.7, p=0.013) and larger debridement size (49.5 versus 17.6 cm2, p=0.0168). Additionally, explantation cases had a much higher rate of ADM/mesh utilization (100% versus 45.5%, p<0.0001), prior radiation (20.0% versus 0%, p=0.0083), immediate implant reconstruction (46.7% versus 20.0%, p=0.0491), concomitant major infection (30.0% versus 1.8%, p=0.028) and both major mastectomy flap and NAC necrosis (33.3% versus 10.9%, p-0.0494). These cases were also more frequently performed in the operating room compared to the office setting (93.3% versus 27.3%, p<0.0001). There were no significant differences between cases requiring explant versus exchange.
Conclusions: NSM cases complicated by ischemia that require explantation have a significantly higher rate of preoperative radiation, immediate implant placement, use of ADM/mesh, concomitant major infection and debridement in an operating room. These variables should be taken into account when discussing risks with patients preoperatively and assessing the quality of mastectomy flaps and subsequent reconstructive choices intraoperatively. 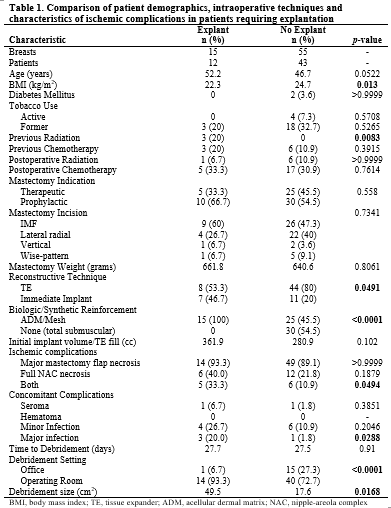
Back to 2019 Abstracts