
Variation in Physician Payments by Anatomical Location in Microsurgery - An All-Payer Claims Database Analysis
Meghana Shamsunder*, MPH1, Clifford Sheckter*, MD2, Avraham Sheinin3, David Rubin3, Nicholas Berlin, MD, MPH4, Evan Matros, MD, MMSc., MPH1.
1Plastic and Reconstructive Surgery Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA, 2Division of Plastic and Reconstructive Surgery, Stanford University Medical Center, Stanford, CA, USA, 3Department of Finance, Memorial Sloan Kettering Cancer Center, New York, NY, USA, 4Section of Plastic Surgery, Department of Surgery, University of Michigan Health System, Ann Arbor, MI, USA.
Background: Microsurgery is a technically challenging discipline, laborious in both time and effort. Work Relative Value Units (wRVU) have been established as a means to standardize reimbursement schemes across a broad spectrum of procedures. This study aims to investigate the payment-to-wRVU ratio for microsurgical and common breast reconstruction procedures based on anatomic location, parsing between commercial and public payers. The hypothesis is that breast reconstruction is associated with the highest payment-to-wRVU ratio compared to other anatomic regions.
Methods: The Massachusetts All-Payer Claims Database was queried from 2010-2014 for microsurgical and breast reconstruction related Current Procedural Terminology (CPT) codes. International Classification of Diseases (ICD) codes were used to categorize procedures by anatomic region. Physician payments were aggregated by anatomic region and per CPT code. Payment-per-wRVU was adjusted for yearly inflation and bilateral procedures. The distribution of payments was described using mean (SD) and median (IQR). Kruskal Wallis tests and Wilcoxon Rank sum tests were used to calculate statistical differences in physician payment-per-wRVU among anatomic regions and CPT codes.
Results: Among 823 commercial claims, breast microsurgical procedures had significantly greater mean and median payments-per-wRVU (median: $121.54 [IQR: 92.01-173.84]) compared to head and neck ($115.05 [74.16-138.64]), trunk ($93.48 [47.15-120.92]), upper extremity ($110.02 [94.55-124.27]), and lower extremity ($112.42 [93.99-142.34]) microsurgical reconstructions (p<0.05). Within commercial breast procedures, physician payments-per-wRVU (p<0.001) were significantly greater only for deep inferior epigastric perforator (DIEP) flaps billed through the Healthcare Common Procedure Coding System (HCPCS) s2068; there were no significant differences in payment among other common breast reconstruction procedures (p=0.446). Among 301 governmental claims, there was no significant difference in physician payment-per-wRVU distributions for lower extremity, head and neck, and breast microsurgical procedures (p=0.103). Within governmental claims, payment-per-wRVU did not differ significantly for common breast reconstruction procedures.
Conclusion: Breast microsurgery procedures reimburse significantly more per wRVU than other anatomic regions for commercial payers. The data also show that physician payment-per-wRVU is comparable for common breast reconstruction procedures with the exception of DIEP flaps billed through HCPCS s2068. The aforementioned findings are nullified when evaluating governmental payers as there is no opportunity for contractual negotiation. 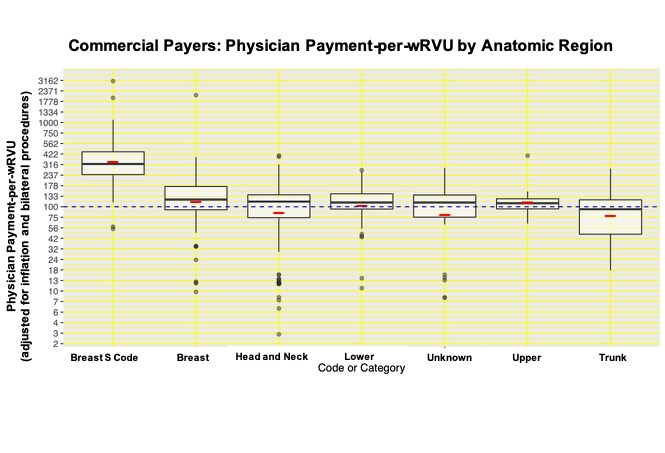
Back to 2019 Abstracts