
Evaluating the Effects of Enhanced Recovery Pathways in Craniosynostosis: National Trends in Hospitalization Charges vs. Length of Stay in Craniosynostosis Surgery
Shannon Wu, Yida Cai, Samuel Boas, Anand Kumar, MD.
Department of Plastic Surgery, University Hospitals Cleveland Medical Center, Cleveland, OH, USA.
BACKGROUND: Enhanced Recovery After Surgery (ERAS) pathways are multimodal approaches aimed at minimizing post-operative surgical stress, reducing hospitalization time, and lowering hospitalization charges. ERAS is broadly and increasingly implemented in hospitals across the country. Early reports have shown ERAS to reduce length of stay (LOS) following commonly performed pediatric surgeries such as pyeloplasty, appendectomy, and bowel anastomosis. However, LOS and hospital charges following craniosynostosis using ERAS has not been studied. Our study analyzes the factors influencing hospital charges relating to craniosynostosis skull procedures and their trends over a multi-year time frame.METHODS: The Healthcare Cost and Utilization Project's (HCUP) National Inpatient Sample (NIS) database was analyzed from January 2009 to December 2014. All patients who were diagnosed with craniosynostosis who underwent skull procedures were included. Variables of interest included demographic data, hospital characteristics, hospitalization data and total hospital charges. Univariate and generalized linear models were used to examine associations between selected variables and the hospitalization charges.RESULTS: 54,583 patients were diagnosed with craniosynostosis between 2009 and 2014. Of these patients, 22,916 (41.9%) received skull surgery and were included. The mean total hospital charge was $81,563.65 (SD=$72,845.57). The mean length of stay (LOS) was 3.8 days (SD=5.0) and there was no significant change in LOS by year (p = 0.979). However, despite no increase in LOS, mean hospitalization charge increased significantly by year (p < 2e-16). Regression analysis showed that the proportion of eligible patients who underwent craniosynostosis skull procedures substantially increased over the selected time frame (p = 0.00328). Regionally, Southern states performed more skull procedures compared to other regions of the US. Most craniosynostosis procedures were performed in urban teaching hospitals and high-volume hospitals. There was no significant association between hospital volume and hospitalization charge (p = 0.331).CONCLUSIONS: Increasing hospital charges despite constant length of stay for craniosynostosis skull procedures was observed between 2009 and 2014. While ERAS has reduced LOS for common pediatric surgical procedures, no decrease in LOS for craniosynostosis has been observed. Further studies to safely lower LOS and hospitalization charges for this procedure would reduce the overall healthcare burden. 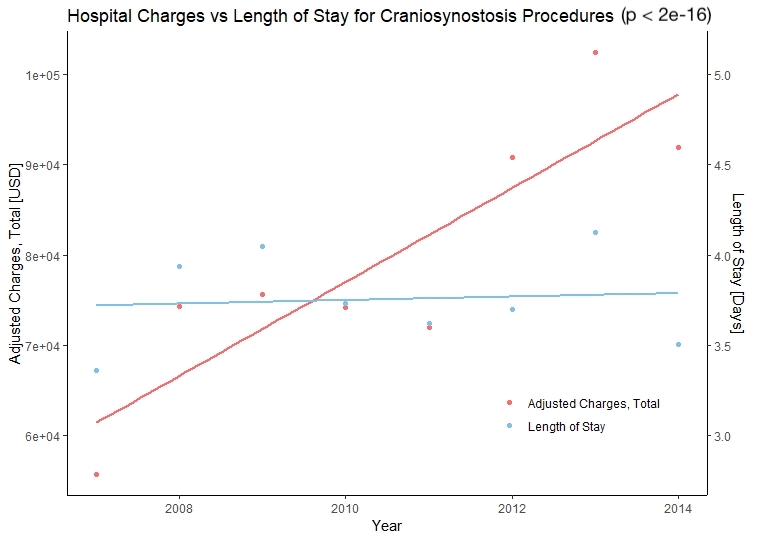
Back to 2020 Abstracts