
Fluid Distribution Patterns in Early Stage Upper Extremity Lymphedema
Rosie Friedman, BS1, Clarissa Lee1, Betsa Parsai Salehi, MD1, Kevin J. Donohoe, MD1, Dhruv Singhal, MD1, Leo Tsai, MD, PhD1
Beth Israel Deaconess Medical Center, Boston, MA
Introduction: Patterns of fluid distribution in mild cases of upper extremity lymphedema have not been widely described and may be important to help determine the presence and location of compensatory lymphatic channels in the upper extremity. The aim of this study was to characterize the spatial distribution of edema in patients with early-stage upper extremity lymphedema.
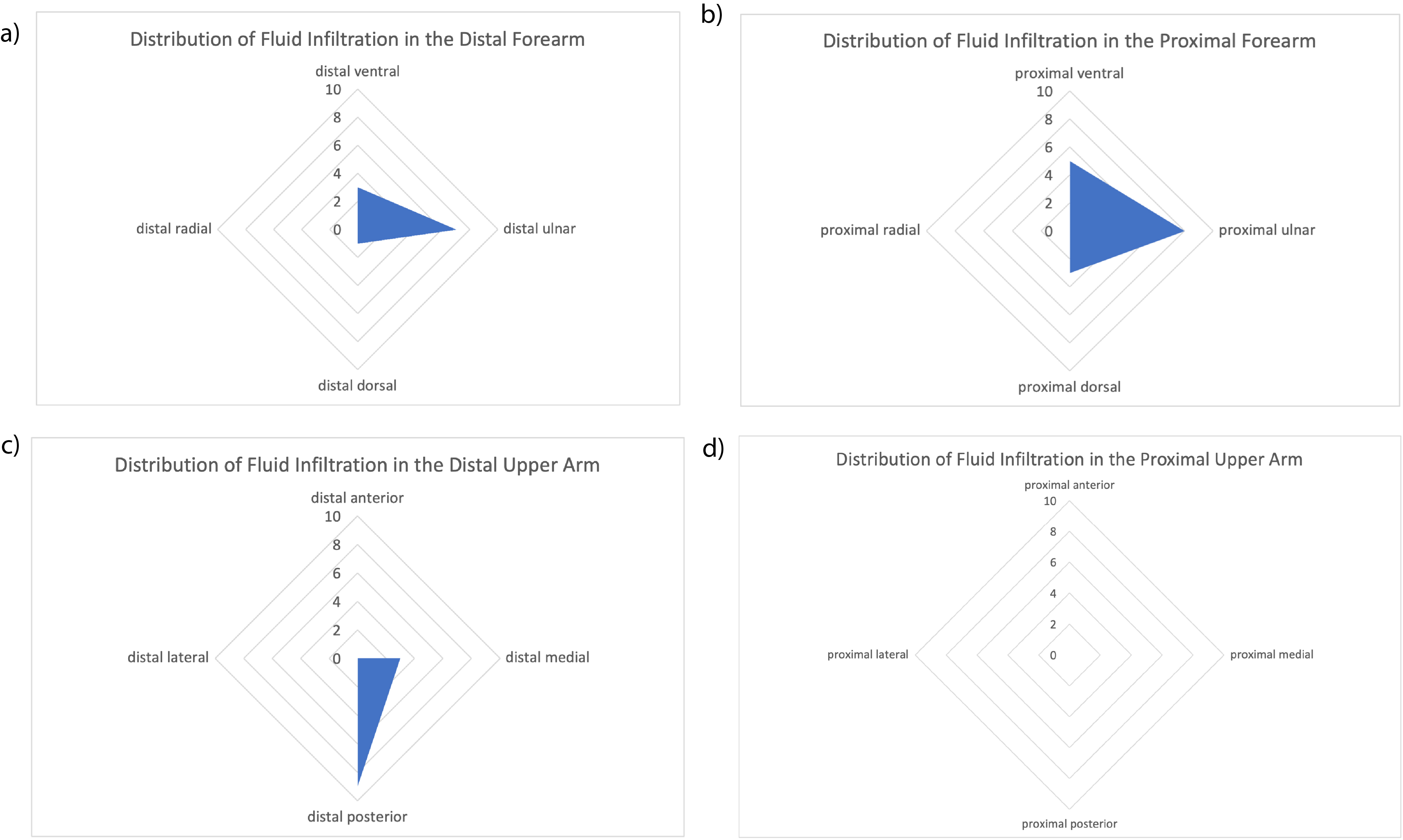
Methods: A retrospective review was conducted to identify patients with MRI stage 1 upper extremity lymphedema, defined as fluid infiltration in the subcutaneous tissue that does not exceed 50% of the circumference of the upper extremity at any level. Using a standardized scoring system, a board-certified radiologist graded the severity and location of fluid infiltration at 5 levels along the extremity: the hand, distal forearm, proximal forearm, distal upper arm and proximal upper arm. A distribution map of edema was created from a summation of the scores across each spatial location for all patients.
Results: Eleven patients with MRI stage 1 upper extremity lymphedema were identified between January 2017 and January 2022. The mean age was 58 years and the mean BMI was 30 m/kg2. One patient had primary lymphedema and the remaining ten patients had secondary lymphedema. In all cases but one, the hand was completely spared. Within the forearm, edema was most prevalent along the ulnar aspect and to a lesser extent the volar forearm. Notably, the radial forearm was not involved. In the upper arm, fluid was primarily concentrated posteriorly and occasionally present medially along the distal portion.
Conclusion: In early-stage lymphedema, fluid infiltration is concentrated along the ulnar forearm and the posterior distal upper arm, which aligns anatomically with the tricipital pathway, with sparing of the radial and lateral aspects, which aligns with the lateral upper arm pathway. Compromise, absence, or unfavorable anatomical variations of tricipital pathway, and relative robustness of the lateral pathway may explain this pattern of fluid distribution in early-stage lymphedema. MRI maps of edema distribution may be used to corroborate lymphatic compromise with other modalities such as indocyanine green lymphangiography.
Back to 2022 Abstracts