
Facial Artery Perforator Flap For Cheek And Midface Reconstruction
Katelyn Lewis, BS,1 Sara Islam, BS2,3, Sarah Phillips, BS2, Martin Carney, MD,3 James Clune, MD,3
1. University of Central Florida College of Medicine, Orlando, FL, USA.2. New York Medical College, Valhalla, NY, USA.3. Division of Plastic and Reconstructive Surgery, Department of Surgery, Yale School of Medicine; New Haven, CT, USA.
Background: Reconstruction of facial melanoma defects can be challenging. Large defects of the midface, cheek and nasolabial fold are often reconstructed using a cervicofacial flap which requires significant flap elevation and undermining. However, local perforator flaps may be used to provide additional skin coverage with less dissection and donor site morbidity. The goal of this study is to evaluate a perforator flap based off of the facial artery and its branches to determine if it is a safe and cosmetically-favorable option to repair oncologic-related defects on the cheek and midface.
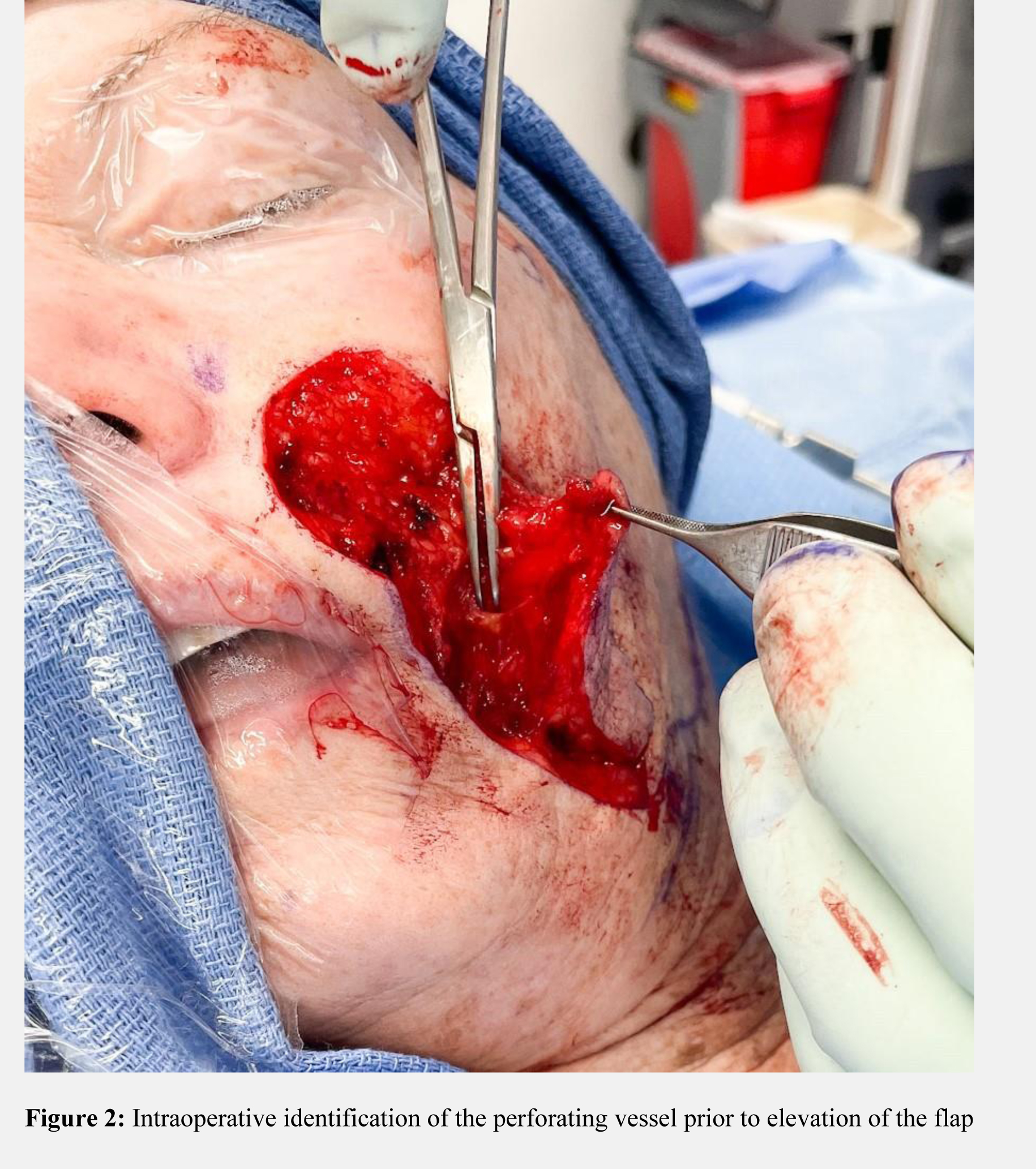
Methods: After institutional review board approval, a retrospective review was performed on patients who underwent melanoma excision and reconstruction with the facial artery perforator flap by the senior author from January 2016 to December 2021. Demographic variables, age, gender, date of surgery, operative logs, medical and surgical history, pathology details, defect and repair size, complications, and length of follow up were recorded. Complications including hematoma, seroma, flap failure, surgical site infection, and dehiscence were recorded. Reoperations were also indicated in cases of complication management and re-excision due to positive margins. Technique: Following melanoma excision, defect dimensions were recorded. Hand-held doppler was used over tissue adjacent to the defect to isolate a perforator. A four-sided flap was designed with the perforator(s) located centrally. The skin was incised and dissected to the platysma muscle. The perforating vessels were identified and resected from the platysma as needed to free the skin, subcutaneous tissue, and muscle 360 degrees around the vascular pedicle. The flap was elevated on the artery and vein of the pedicle and inset into the defect site.
Results: 16 patients were included in our cohort. The average age was 67.3 years and 53% (n=8) were female. Fourteen patients had the primary defect located on the cheek, 1 from the nasolabial fold, and 1 from the lateral nasal bridge. All patients received immediate reconstruction. Excisional margins ranged from 0.5 to 2 cm. Two patients had positive margins following pathology results with one undergoing treatment with imiquimod and the other opting for close follow-up. No complications involving the defect or donor site were reported after an average follow-up time of 113.8 days.
Conclusion: The facial artery perforator flap is a safe and cosmetically-favorable option to repair oncologic-related defects on the cheek and midface. There is less donor site morbidity and less facial dissection compared to alternatives such as the cervicofacial flap.



Back to 2022 Abstracts