
Let's Discuss Babysitters: A Timeline of Sensory Return in Delayed-Immediate Neurotized DIEP Flap Reconstruction
Marcos Lu Wang BA1, Hao Huang MD2, Nancy Qin BA1, Angela Ellison MS1, Paul A. Asadourian MEng3, David M. Otterburn MD1
1Weill Cornell Medicine, New York, NY; 2NewYork-Presbyterian Hospital, New York, NY; 3 Columbia University Irving Medical Center, New York, NY
Background: Breast reconstruction patients who are anticipated to undergo adjuvant radiation are not suitable candidates for immediate deep inferior epigastric perforator (DIEP) flap reconstruction due to the risk of flap fibrosis, shrinkage, and fat necrosis. Rather, many of these patients undergo delayed-immediate, or babysitter, reconstruction, where a tissue expander is placed first as a temporizing measure during adjuvant therapy before definitive flap reconstruction. In our previous study of breast sensory recovery, we demonstrated that neurotized DIEP flap reconstruction yields superior sensory return compared to implant-based reconstruction. In this study, we aim to delineate the temporal pattern of sensory changes in babysitter patients following final-stage neurotized flap reconstruction.
Methods: Ninety-one patients who underwent mastectomy with immediate reconstruction, including 26 patients (46 breasts) with babysitter procedures and 65 patients (120 breasts) with immediate DIEP flaps, were prospectively identified at their pre-operative visit. For both cohorts, baseline level (t = 0) is defined as prior to mastectomy. Sensitivity evaluation was performed in nine breast regions, utilizing the AcroVal pressure-specified sensory device to determine 1-point static cutaneous thresholds at which stimulus was perceived. Higher thresholds indicated worse sensitivity. Sensitivity data was averaged between patients at each time point, plotted over time, and compared between babysitter and DIEP groups.
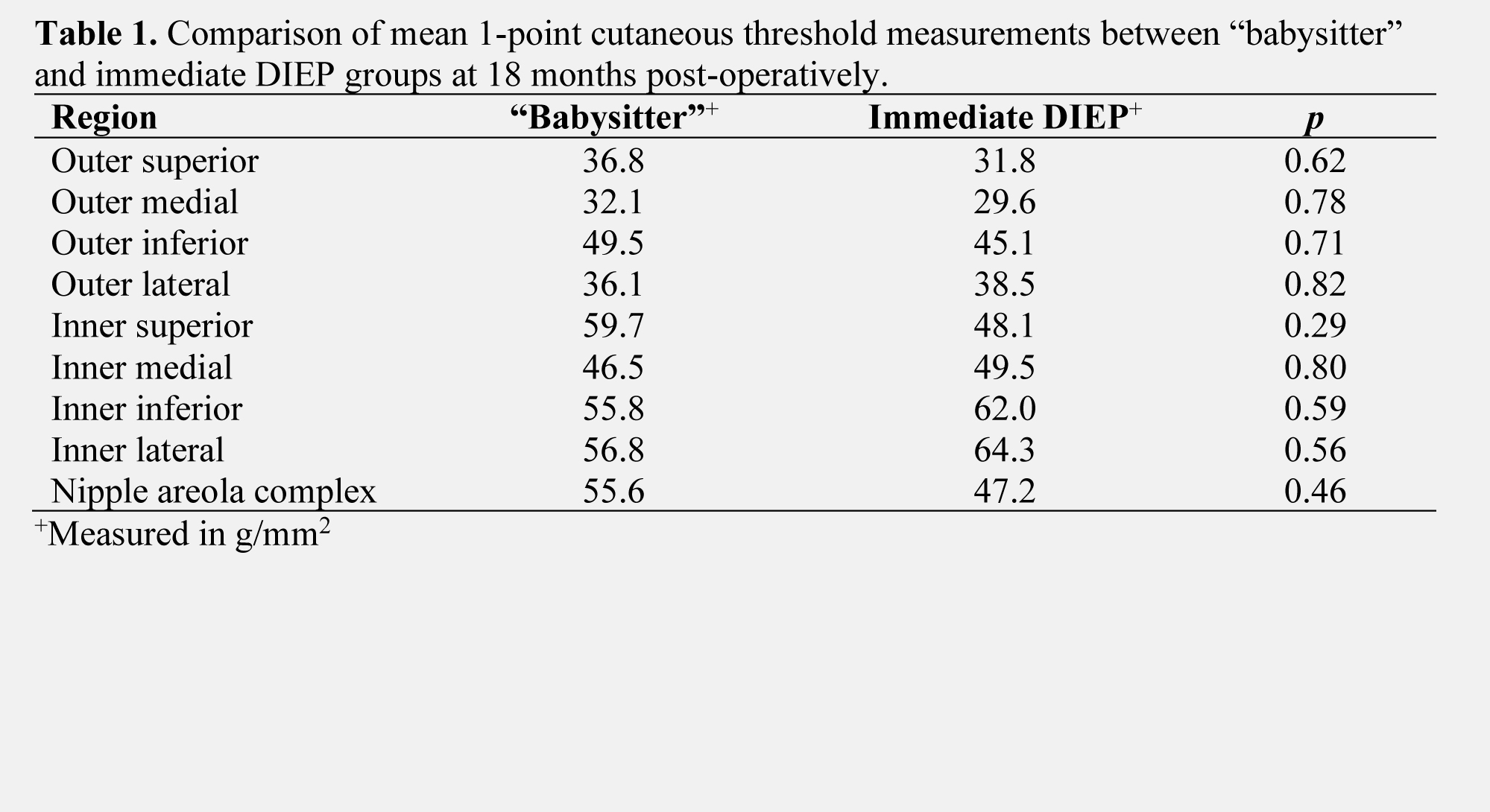
Results: Babysitter patients underwent final-stage neurotized flap reconstruction on average at 12 months following mastectomy and initial tissue expander placement (range, 3 to 18 months). At 18 months post-mastectomy (6 months post-DIEP), babysitter patients had comparable sensitivity measurements as immediate DIEP flap patients in all regions of the breast (p > 0.05 for all breast regions, Table 1). For babysitter patients, at 18 months post-operatively, sensitivity measurements were comparable to baseline levels only in the outer superior, outer medial, and outer lateral regions of the breast (p > 0.05). At 24 months post-operatively, cutaneous thresholds were comparable to baseline in all regions of the breast except the inner inferior region (p > 0.05), following a similar sensory recovery trajectory as immediate neurotized DIEP flap patients.
Conclusions: In patients who undergo babysitter procedures, the combination of sensory return from the native mastectomy skin flap along with the neurotized DIEP flap yields sensory recovery comparable to immediate DIEP flap patients following definitive flap reconstruction. When final-stage flap reconstruction occurs by 12 months post-mastectomy, sensation can return beginning 24 months postoperatively, or even sooner in some regions of the breast.
Back to 2022 Abstracts